

Racial/Ethnic and Geographic Disparities in Comorbid Traumatic Brain Injury-Renal Failure in US Veterans and Associated Veterans Affairs Resource Costs, 2000-2020
- PMID: 36864369
- PMCID: PMC10474245
- DOI: 10.1007/s40615-023-01550-4
Racial/Ethnic and Geographic Disparities in Comorbid Traumatic Brain Injury-Renal Failure in US Veterans and Associated Veterans Affairs Resource Costs, 2000-2020
Abstract
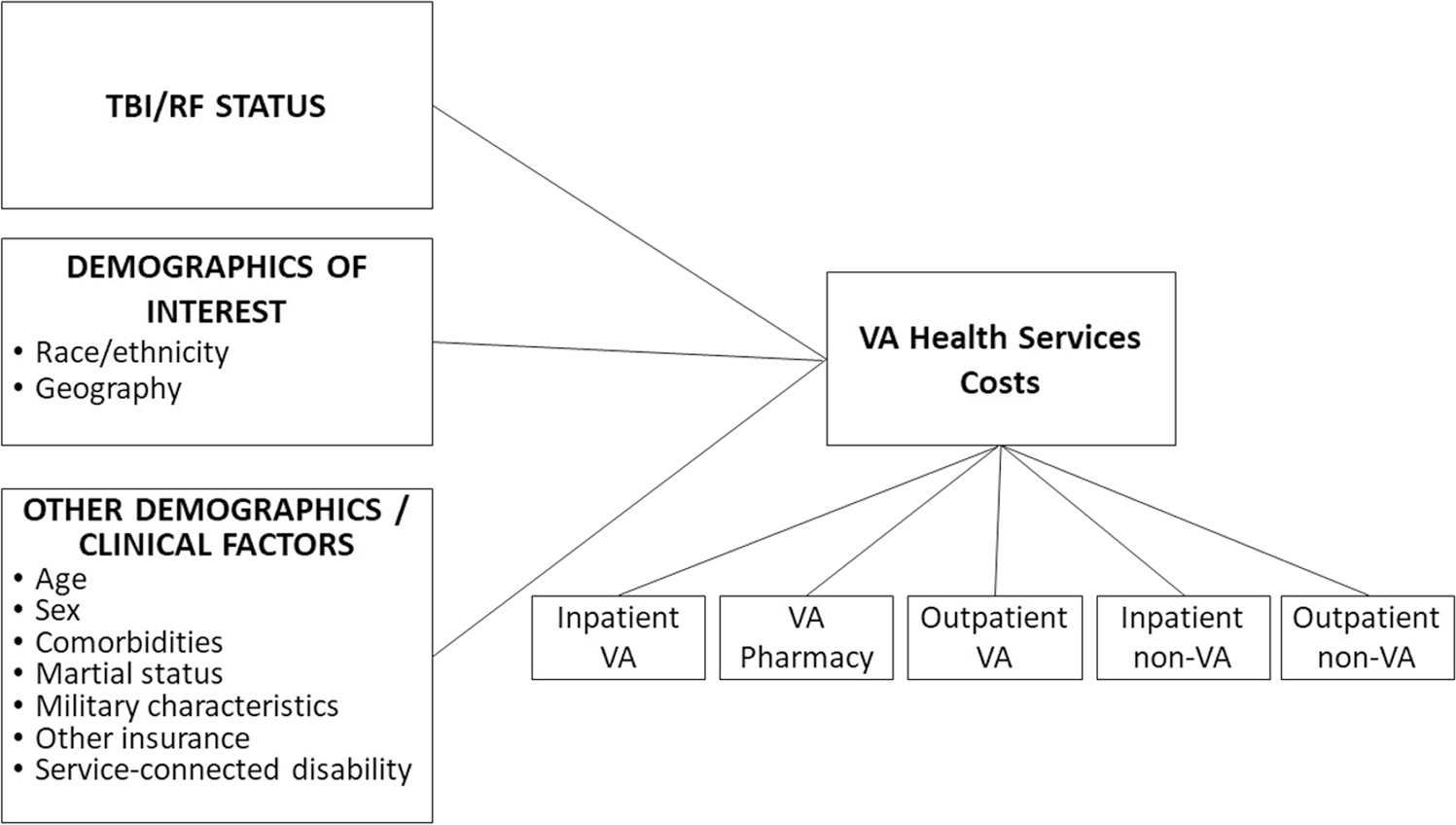
Studies have identified disparities by race/ethnicity and geographic status among veterans with traumatic brain injury (TBI) and renal failure (RF). We examined the association of race/ethnicity and geographic status with RF onset in veterans with and without TBI, and the impact of disparities on Veterans Health Administration resource costs.
Methods: Demographics by TBI and RF status were assessed. We estimated Cox proportional hazards models for progression to RF and generalized estimating equations for inpatient, outpatient, and pharmacy cost annually and time since TBI + RF diagnosis, stratified by age.
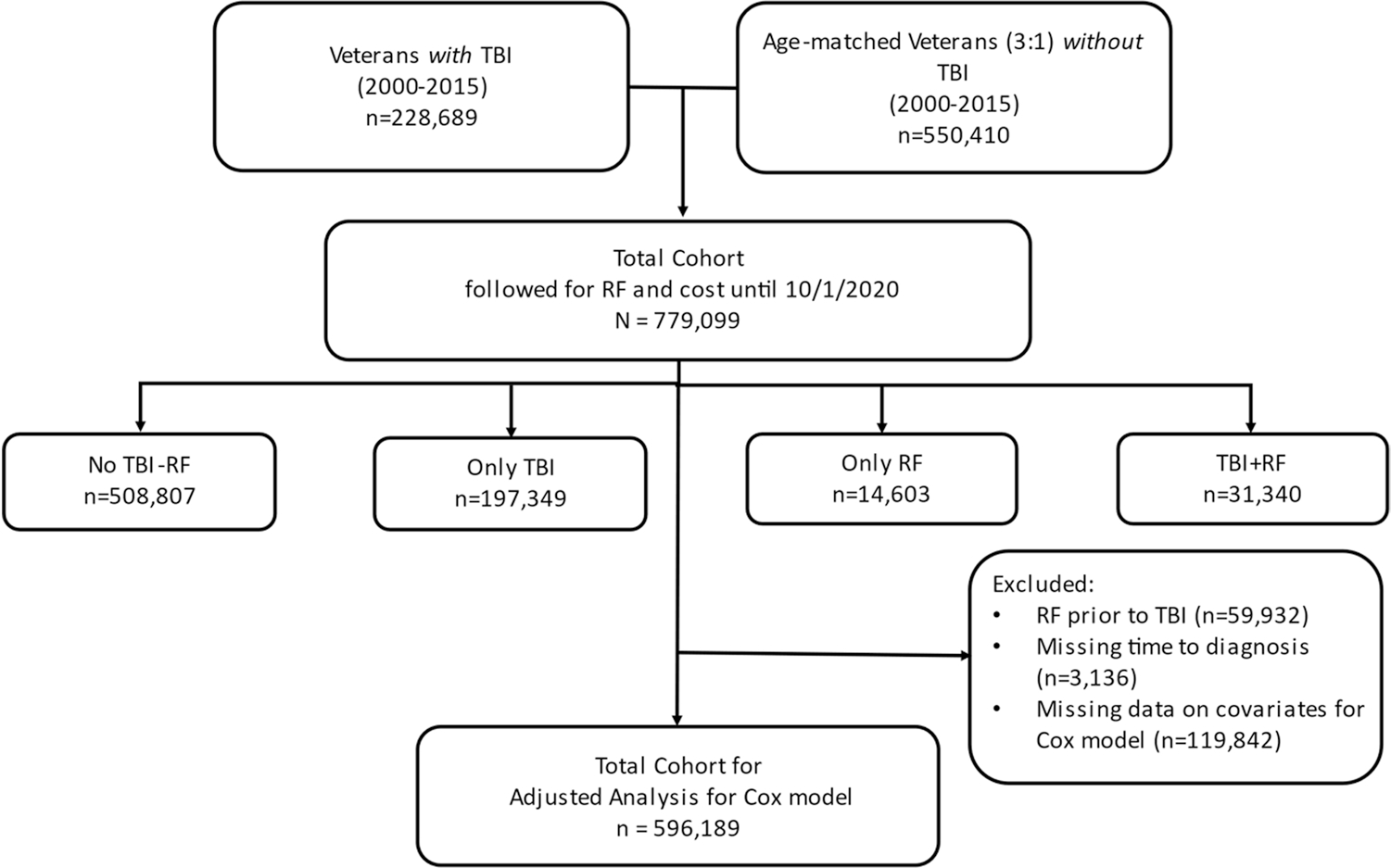
Results: Among 596,189 veterans, veterans with TBI progressed faster to RF than those without TBI (HR 1.96). Non-Hispanic Black veterans (HR 1.41) and those in US territories (HR 1.71) progressed faster to RF relative to non-Hispanic Whites and those in urban mainland areas. Non-Hispanic Blacks (-$5,180), Hispanic/Latinos ($-4,984), and veterans in US territories (-$3,740) received fewer annual total VA resources. This was true for all Hispanic/Latinos, while only significant for non-Hispanic Black and US territory veterans < 65 years. For veterans with TBI + RF, higher total resource costs only occurred ≥ 10 years after TBI + RF diagnosis ($32,361), independent of age. Hispanic/Latino veterans ≥ 65 years received $8,248 less than non-Hispanic Whites and veterans living in US territories < 65 years received $37,514 less relative to urban veterans.
Conclusion: Concerted efforts to address RF progression in veterans with TBI, especially in non-Hispanic Blacks and those in US territories, are needed. Importantly, culturally appropriate interventions to improve access to care for these groups should be a priority of the Department of Veterans Affairs priority for these groups.
© 2023. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Figures
Similar articles
-
Racial/Ethnic disparities in mortality risk among US veterans with traumatic brain injury.Am J Public Health. 2012 May;102 Suppl 2(Suppl 2):S266-71. doi: 10.2105/AJPH.2011.300176. Epub 2011 Nov 28. Am J Public Health. 2012. PMID: 21852658 Free PMC article.
-
Racial/Ethnic Disparities in VA Services Utilization as a Partial Pathway to Mortality Differentials Among Veterans Diagnosed With TBI.Glob J Health Sci. 2015 Jul 19;8(2):260-72. doi: 10.5539/gjhs.v8n2p260. Glob J Health Sci. 2015. PMID: 26383194 Free PMC article.
-
Sociodemographic and Health Characteristics of Hispanic Veteran Patients With Traumatic Brain Injury and Its Association to Mortality: A Pilot Study.Mil Med. 2025 Jan 16;190(1-2):157-164. doi: 10.1093/milmed/usae346. Mil Med. 2025. PMID: 39042559
-
Racial/Ethnic Differences in Traumatic Brain Injury: Pathophysiology, Outcomes, and Future Directions.J Neurotrauma. 2023 Mar;40(5-6):502-513. doi: 10.1089/neu.2021.0455. Epub 2022 Sep 29. J Neurotrauma. 2023. PMID: 36029219 Review.
-
Neuroimaging and Neurophysiologic Biomarkers for Mental Health: An Evidence Map [Internet].Washington (DC): Department of Veterans Affairs (US); 2022 Oct. Washington (DC): Department of Veterans Affairs (US); 2022 Oct. PMID: 37192328 Free Books & Documents. Review.
References
-
- Centers for Disease Control and Prevention. Report to Congress on Traumatic Brain Injury in the United States: Epidemiology and Rehabilitation. National Center for Injury Prevention and Control. Division of Unintentional Injury Prevention. Atlanta, GA; 2015.
-
- Centers for Disease Control and Prevention. Surveillance Report of Traumatic Brain Injury-related Deaths by Age Group, Sex, and Mechanism of Injury—United States, 2018 and 2019. Centers for Disease Control and Prevention, U.S. Department of Health and Human Services; 2022.
Publication types
MeSH terms
Grants and funding
- I01 RX002174/RX/RRD VA/United States
- I01 RX003444/RX/RRD VA/United States
- I01 RX003442/RX/RRD VA/United States
- I01 CX001135/CX/CSRD VA/United States
- I01 RX003443/RX/RRD VA/United States
- I01 RX001880/RX/RRD VA/United States
- I01 RX002171/RX/RRD VA/United States
- I01 HX003155/HX/HSRD VA/United States
- I01 RX002076/RX/RRD VA/United States
- K24 DK093699/DK/NIDDK NIH HHS/United States
- I01 CX001246/CX/CSRD VA/United States
- I01 RX002173/RX/RRD VA/United States
- R01 DK118038/DK/NIDDK NIH HHS/United States
- I01 RX001135/RX/RRD VA/United States
- I01 RX002172/RX/RRD VA/United States
- K23 MD016448/MD/NIMHD NIH HHS/United States
- I01 RX001774/RX/RRD VA/United States
- I01 CX002097/CX/CSRD VA/United States
- I01 RX002170/RX/RRD VA/United States
- R01 DK120861/DK/NIDDK NIH HHS/United States
- I01 CX002096/CX/CSRD VA/United States
- R01 MD013826/MD/NIMHD NIH HHS/United States
- R21 DK131356/DK/NIDDK NIH HHS/United States
- KL2 TR001438/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical