

Improving vasopressor use in cardiac arrest
- PMID: 36864469
- PMCID: PMC9979497
- DOI: 10.1186/s13054-023-04301-3
Improving vasopressor use in cardiac arrest
Abstract
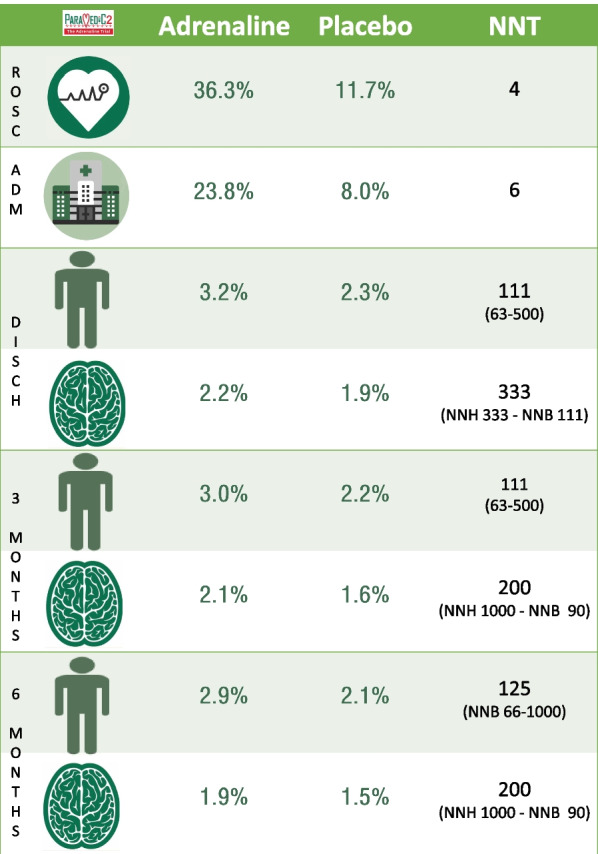
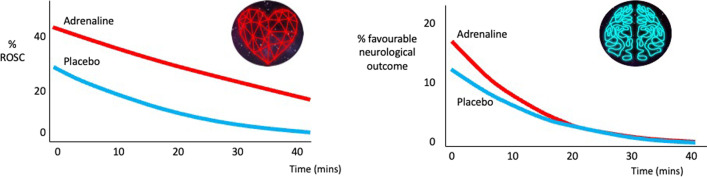
The Chain of Survival highlights the effectiveness of early recognition of cardiac arrest and call for help, early cardiopulmonary resuscitation and early defibrillation. Most patients, however, remain in cardiac arrest despite these interventions. Drug treatments, particularly the use of vasopressors, have been included in resuscitation algorithms since their inception. This narrative review describes the current evidence base for vasopressors and reports that adrenaline (1 mg) is highly effective at achieving return of spontaneous circulation (number needed to treat 4) but is less effective on long-term outcomes (survival to 30 days, number needed to treat 111) with uncertain effects on survival with a favourable neurological outcome. Randomised trials evaluating vasopressin, either as an alternative to or in addition to adrenaline, and high-dose adrenaline have failed to find evidence of improved long-term outcomes. There is a need for future trials to evaluate the interaction between steroids and vasopressin. Evidence for other vasopressors (e.g. noradrenaline, phenylephedrine) is insufficient to support or refute their use. The use of intravenous calcium chloride as a routine intervention in out of hospital cardiac arrest is not associated with benefit and may cause harm. The optimal route for vascular access between peripheral intravenous versus intraosseous routes is currently the subject of two large randomised trials. Intracardiac, endobronchial, and intramuscular routes are not recommended. Central venous administration should be limited to patients where an existing central venous catheter is in situ and patent.
Keywords: Adrenaline; Advanced life support drugs; Cardiac arrest; Vasopressin; Vasopressors.
© 2023. The Author(s).
Conflict of interest statement
GDP - Chief investigator for the PARAMEDIC2 and PARAMEDIC3 which were funded by the National Institute for Health and Care Research. Editor roles with the journals Resuscitation and Resuscitation Plus. Volunteer roles with the European Resuscitation Council, Resuscitation Council UK and International Liaison Committee on Resuscitation. KC- Co-investigator for the PARAMEDIC3 trial, which is funded by the National Institute for Health and Care Research. Associate Editor for Resuscitation Plus. Volunteer roles with the European Resuscitation Council, Resuscitation Council UK and International Liaison Committee on Resuscitation.
Figures
References
-
- Perkins GD, Jacobs IG, Nadkarni VM, Berg RA, Bhanji F, Biarent D, Bossaert LL, Brett SJ, Chamberlain D, de Caen AR, et al. Cardiac arrest and cardiopulmonary resuscitation outcome reports: update of the Utstein resuscitation registry templates for out-of-hospital cardiac arrest. Resuscitation. 2014;96:328–340. doi: 10.1016/j.resuscitation.2014.11.002. - DOI - PubMed
-
- Kiguchi T, Okubo M, Nishiyama C, Maconochie I, Ong MEH, Kern KB, Wyckoff MH, McNally B, Christensen EF, Tjelmeland I, et al. Out-of-hospital cardiac arrest across the World: first report from the International Liaison Committee on Resuscitation (ILCOR) Resuscitation. 2020;152:39–49. doi: 10.1016/j.resuscitation.2020.02.044. - DOI - PubMed
-
- Safar P, Bircher NG. Cardiopulmonary cerebral resuscitation. London: Laerdal Medical; 1968.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
