

Comparison of liver fibrosis scores for predicting mortality and morbidity in heart failure with preserved ejection fraction
- PMID: 36864701
- PMCID: PMC10192244
- DOI: 10.1002/ehf2.14336
Comparison of liver fibrosis scores for predicting mortality and morbidity in heart failure with preserved ejection fraction
Abstract
Aims: Liver fibrosis scores (LFSs) are non-invasive and effective tools for estimating cardiovascular risks. To better understand the advantages and limitations of currently available LFSs, we determined to compare the predictive values of LFSs in heart failure with preserved ejection fraction (HFpEF) for primary composite outcome, atrial fibrillation (AF), and other clinical outcomes.
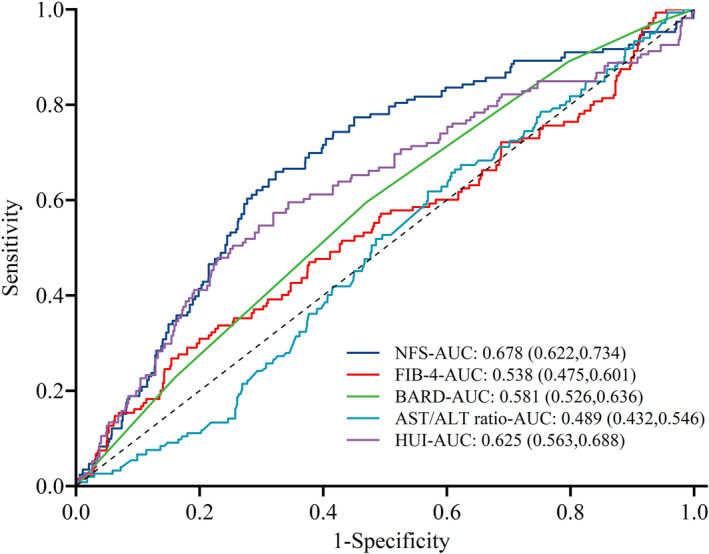
Methods and results: This was a secondary analysis of the TOPCAT trial, and 3212 HFpEF patients were enrolled. Five LFSs, namely, non-alcoholic fatty liver disease fibrosis score (NFS), fibrosis-4 score (FIB-4), BARD, aspartate aminotransferase (AST)/alanine aminotransferase (ALT) ratio, and Health Utilities Index (HUI) scores were adopted. Cox proportional hazard model and competing risk regression model were performed to assess the associations between LFSs and outcomes. The discriminatory power of each LFS was evaluated by calculating the area under the curves (AUCs). During a median follow-up of 3.3 years, a 1-point increase in the NFS [hazard ratio (HR) 1.10; 95% confidence interval (CI) 1.04-1.17], BARD (HR 1.19; 95% CI 1.10-1.30), and HUI (HR 1.44; 95% CI 1.09-1.89) scores was associated with an increased risk of primary outcome. Patients with high levels of NFS (HR 1.63; 95% CI 1.26-2.13), BARD (HR 1.64; 95% CI 1.25-2.15), AST/ALT ratio (HR 1.30; 95% CI 1.05-1.60), and HUI (HR 1.25; 95% CI 1.02-1.53) were at an increased risk of primary outcome. Subjects who developed AF were more likely to have high NFS (HR 2.21; 95% CI 1.13-4.32). High levels of NFS and HUI scores were a significant predictor of any hospitalization and hospitalization for heart failure. The AUCs for the NFS in predicting primary outcome (0.672; 95% CI 0.642-0.702) and incident of AF (0.678; 95% CI 0.622-0.734) were higher than other LFSs.
Conclusions: In light of these findings, NFS appears to have superior predictive and prognostic utility compared with AST/ALT ratio, FIB-4, BARD, and HUI scores.
Clinical trial registration: (https://clinicaltrials.gov). Unique identifier: NCT00094302.
Keywords: Adverse outcomes; Heart failure with preserved ejection fraction; Liver fibrosis score.
© 2023 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
All authors declare that they have no conflict of interest.
Figures


Similar articles
-
Association of liver fibrosis scores with all-cause and cardiovascular mortality in patients with heart failure.Clin Transl Sci. 2024 Dec;17(12):e70104. doi: 10.1111/cts.70104. Clin Transl Sci. 2024. PMID: 39686669 Free PMC article.
-
Liver fibrosis scores and atrial fibrillation incidence in heart failure with preserved ejection fraction.ESC Heart Fail. 2022 Dec;9(6):3985-3994. doi: 10.1002/ehf2.14087. Epub 2022 Aug 22. ESC Heart Fail. 2022. PMID: 35996808 Free PMC article.
-
Association of liver fibrosis risk scores with clinical outcomes in patients with heart failure with preserved ejection fraction: findings from TOPCAT.ESC Heart Fail. 2021 Apr;8(2):842-848. doi: 10.1002/ehf2.13250. Epub 2021 Feb 14. ESC Heart Fail. 2021. PMID: 33586354 Free PMC article.
-
FIB-4 stage of liver fibrosis is associated with incident heart failure with preserved, but not reduced, ejection fraction among people with and without HIV or hepatitis C.Prog Cardiovasc Dis. 2020 Mar-Apr;63(2):184-191. doi: 10.1016/j.pcad.2020.02.010. Epub 2020 Feb 15. Prog Cardiovasc Dis. 2020. PMID: 32068085 Free PMC article. Review.
-
Liver fibrosis scores and prognosis in patients with cardiovascular diseases: A systematic review and meta-analysis.Eur J Clin Invest. 2022 Nov;52(11):e13855. doi: 10.1111/eci.13855. Epub 2022 Sep 7. Eur J Clin Invest. 2022. PMID: 36001034
Cited by
-
Association of liver fibrosis scores with all-cause and cardiovascular mortality in patients with heart failure.Clin Transl Sci. 2024 Dec;17(12):e70104. doi: 10.1111/cts.70104. Clin Transl Sci. 2024. PMID: 39686669 Free PMC article.
-
Biomarkers of Hepatic Dysfunction and Cardiovascular Risk.Curr Cardiol Rep. 2023 Dec;25(12):1783-1795. doi: 10.1007/s11886-023-01993-5. Epub 2023 Nov 16. Curr Cardiol Rep. 2023. PMID: 37971635 Free PMC article. Review.
-
Aspartate aminotransferase to alanine aminotransferase ratio and short-term prognosis of patients with type 2 diabetes hospitalized for heart failure.Arch Med Sci. 2024 Oct 22;20(5):1416-1425. doi: 10.5114/aoms/184153. eCollection 2024. Arch Med Sci. 2024. PMID: 39649287 Free PMC article.
-
Association of Non-Invasive Markers with Significant Fibrosis in Patients with Nonalcoholic Fatty Liver Disease: A Cross-Sectional Study.Diabetes Metab Syndr Obes. 2023 Jul 31;16:2255-2268. doi: 10.2147/DMSO.S417754. eCollection 2023. Diabetes Metab Syndr Obes. 2023. PMID: 37545743 Free PMC article.
-
Association Between the Liver Fibrosis Markers and Scores, and Hemodynamic Congestion Assessed by Peripheral Venous Pressure in Patients With Acute Heart Failure.J Am Heart Assoc. 2023 Nov 7;12(21):e030788. doi: 10.1161/JAHA.123.030788. Epub 2023 Nov 6. J Am Heart Assoc. 2023. PMID: 37929710 Free PMC article.
References
-
- McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, Burri H, Butler J, Čelutkienė J, Chioncel O, Cleland JGF, Coats AJS, Crespo‐Leiro MG, Farmakis D, Gilard M, Heymans S, Hoes AW, Jaarsma T, Jankowska EA, Lainscak M, Lam CSP, Lyon AR, McMurray JJV, Mebazaa A, Mindham R, Muneretto C, Francesco Piepoli M, Price S, Rosano GMC, Ruschitzka F, Kathrine Skibelund A, ESC Scientific Document Group , de Boer RA, Christian Schulze P, Abdelhamid M, Aboyans V, Adamopoulos S, Anker SD, Arbelo E, Asteggiano R, Bauersachs J, Bayes‐Genis A, Borger MA, Budts W, Cikes M, Damman K, Delgado V, Dendale P, Dilaveris P, Drexel H, Ezekowitz J, Falk V, Fauchier L, Filippatos G, Fraser A, Frey N, Gale CP, Gustafsson F, Harris J, Iung B, Janssens S, Jessup M, Konradi A, Kotecha D, Lambrinou E, Lancellotti P, Landmesser U, Leclercq C, Lewis BS, Leyva F, Linhart A, Løchen ML, Lund LH, Mancini D, Masip J, Milicic D, Mueller C, Nef H, Nielsen JC, Neubeck L, Noutsias M, Petersen SE, Sonia Petronio A, Ponikowski P, Prescott E, Rakisheva A, Richter DJ, Schlyakhto E, Seferovic P, Senni M, Sitges M, Sousa‐Uva M, Tocchetti CG, Touyz RM, Tschoepe C, Waltenberger J, Adamo M, Baumbach A, Böhm M, Burri H, Čelutkienė J, Chioncel O, Cleland JGF, Coats AJS, Crespo‐Leiro MG, Farmakis D, Gardner RS, Gilard M, Heymans S, Hoes AW, Jaarsma T, Jankowska EA, Lainscak M, Lam CSP, Lyon AR, McMurray JJV, Mebazaa A, Mindham R, Muneretto C, Piepoli MF, Price S, Rosano GMC, Ruschitzka F, Skibelund AK. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021; 42: 3599–3726. - PubMed
-
- Miranda‐Silva D, Lima T, Rodrigues P, Leite‐Moreira A, Falcão‐Pires I. Mechanisms underlying the pathophysiology of heart failure with preserved ejection fraction: the tip of the iceberg. Heart Fail Rev. 2021; 26: 453–478. - PubMed
-
- Ather S, Chan W, Bozkurt B, Aguilar D, Ramasubbu K, Zachariah AA, Wehrens XHT, Deswal A. Impact of noncardiac comorbidities on morbidity and mortality in a predominantly male population with heart failure and preserved versus reduced ejection fraction. J Am Coll Cardiol. 2012; 59: 998–1005. - PMC - PubMed
-
- Campbell RT, Jhund PS, Castagno D, Hawkins NM, Petrie MC, McMurray JJ. What have we learned about patients with heart failure and preserved ejection fraction from DIG‐PEF, CHARM‐preserved, and I‐PRESERVE? J Am Coll Cardiol. 2012; 60: 2349–2356. - PubMed
-
- Loomba R, Friedman SL, Shulman GI. Mechanisms and disease consequences of nonalcoholic fatty liver disease. Cell. 2021; 184: 2537–2564. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
