

A comparative post hoc analysis of finerenone and spironolactone in resistant hypertension in moderate-to-advanced chronic kidney disease
- PMID: 36864892
- PMCID: PMC9972517
- DOI: 10.1093/ckj/sfac234
A comparative post hoc analysis of finerenone and spironolactone in resistant hypertension in moderate-to-advanced chronic kidney disease
Abstract
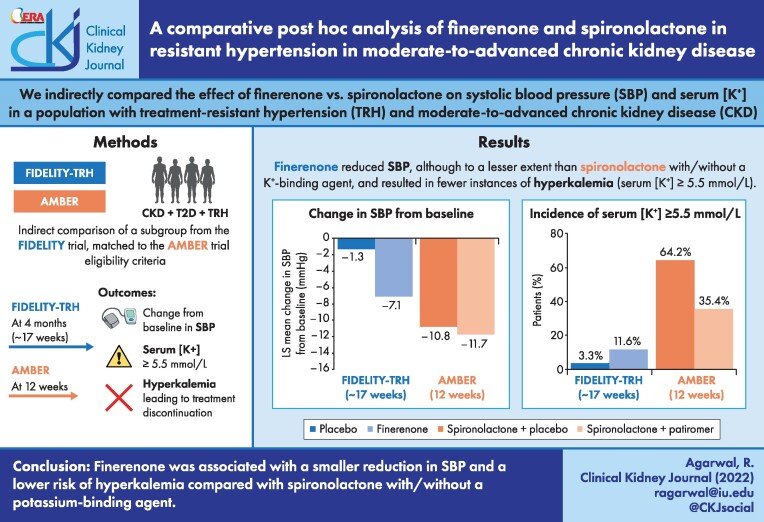
Background: Mineralocorticoid receptor antagonists (MRAs) reduce systolic blood pressure (SBP) and increase serum potassium concentration ([K+]). This indirect comparison investigated any differences in SBP-lowering and hyperkalemia risk between finerenone, a nonsteroidal MRA, and the steroidal MRA spironolactone ± a potassium binder.
Methods: In FIDELITY (a pooled analysis of FIDELIO-DKD and FIGARO-DKD), a subgroup of patients with treatment-resistant hypertension (TRH) and chronic kidney disease meeting eligibility criteria of the AMBER trial were identified (FIDELITY-TRH). The main outcomes were mean change in SBP, incidence of serum [K+] ≥5.5 mmol/L and hyperkalemia-associated treatment discontinuation. Results at ∼17 weeks were compared with 12 weeks from AMBER.
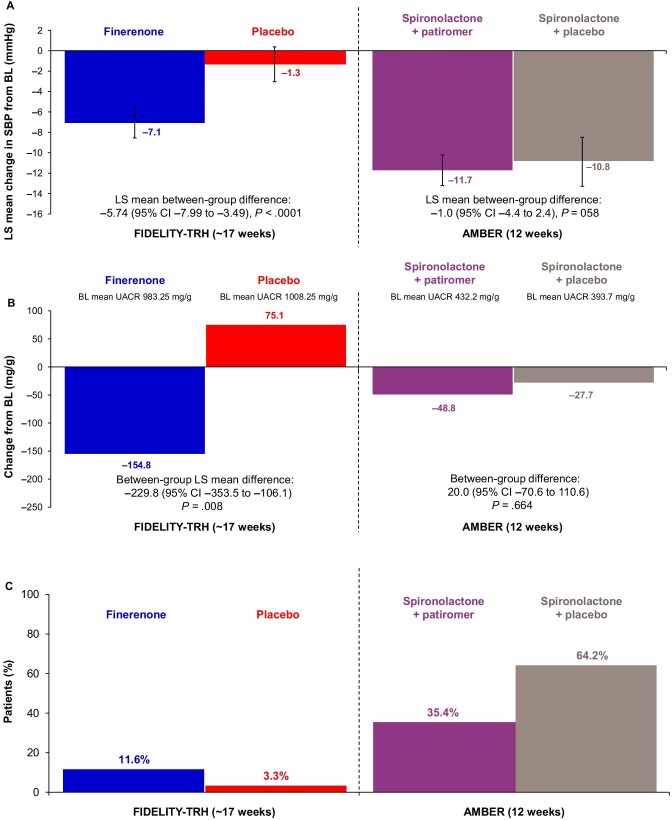
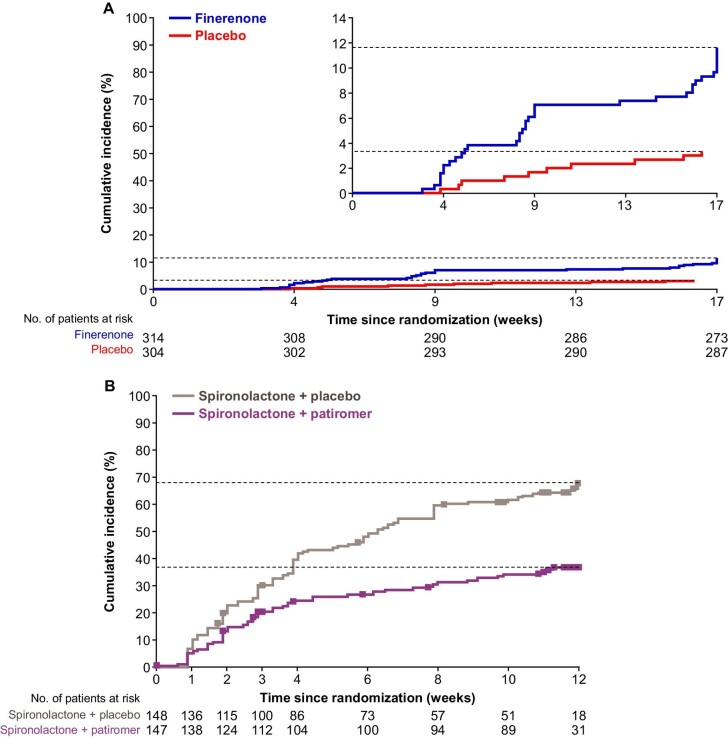
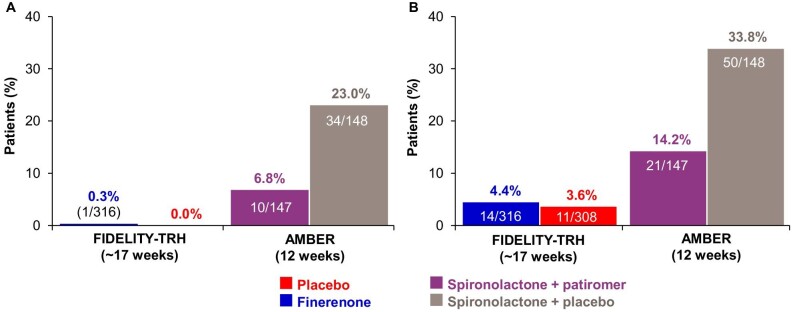
Results: In 624 FIDELITY-TRH patients and 295 AMBER patients, the least squares mean change in SBP (mmHg) from baseline was -7.1 for finerenone and -1.3 for placebo {between-group difference -5.74 [95% confidence interval (CI) -7.99 to -3.49], P < .0001} versus -11.7 for spironolactone + patiromer and -10.8 for spironolactone + placebo [between-group difference -1.0 (95% CI -4.4-2.4), P = .58]. The incidence of serum [K+] ≥5.5 mmol/L was 12% for finerenone and 3% for placebo versus 35% with spironolactone + patiromer and 64% with spironolactone + placebo. Treatment discontinuation due to hyperkalemia was 0.3% for finerenone and 0% for placebo versus 7% for spironolactone + patiromer and 23% for spironolactone + placebo.
Conclusions: In patients with TRH and chronic kidney disease compared with spironolactone with or without patiromer, finerenone was associated with a lower SBP reduction and lower risk of hyperkalemia and treatment discontinuation.Trial Registration: AMBER (NCT03071263), FIDELIO-DKD (NCT02540993), FIGARO-DKD (NCT02545049).
Keywords: finerenone; hyperkalemia; hypertension; patiromer; spironolactone.
© The Author(s) 2022. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
R.A. has received personal fees and nonfinancial support from Bayer Healthcare Pharmaceuticals during the conduct of the study; personal fees and nonfinancial support from Akebia Therapeutics, AstraZeneca, Boehringer Ingelheim, Eli Lilly and Vifor Pharma; is a member of data safety monitoring committees for Chinook and Vertex; served as associate editor of the
S.D.A. has received research support from Abbott Vascular and Vifor International and personal fees from Abbott Vascular, Bayer, Boehringer Ingelheim, BRAHMS, Cardiac Dimensions, Impulse Dynamics, Novartis, Servier and Vifor Pharma.
G.F. is a committee member of trials and registries sponsored by Amgen, Bayer, Boehringer Ingelheim, Medtronic, Novartis, Servier and Vifor Pharma and is senior consulting editor for
P.R. has received personal fees from Bayer during the conduct of the study, research support and personal fees from AstraZeneca and Novo Nordisk and personal fees from Astellas, Boehringer Ingelheim, Eli Lilly, Gilead, Mundipharma, Sanofi and Vifor; all fees are given to Steno Diabetes Center Copenhagen.
L.M.R. has received consultancy fees from Bayer.
B.P. has received consultancy fees for AstraZeneca, Bayer, Boehringer Ingelheim, Brainstorm Medical, Cereno Scientific, G3 Pharmaceuticals, KBP Biosciences, PhaseBio, Proton Intel, Sanofi/Lexicon, Sarfez, scPharmaceuticals, SQ Innovation, Tricida and Vifor/Relypsa; has stock options for KBP Biosciences, Brainstorm Medical, Cereno Scientific, G3 Pharmaceuticals, Proton Intel, Sarfez, scPharmaceuticals, SQ Innovation, Tricida and Vifor/Relypsa and holds a patent for site-specific delivery of eplerenone to the myocardium (US patent 9931412) and a provisional patent for histone acetylation-modulating agents for the treatment and prevention of organ injury (provisional patent US 63/045784).
C.K. has received consultancy fees from Abbott, Akebia, AstraZeneca, Bayer, Boehringer Ingelheim, Cara Therapeutics, CSL Behring, Rockwell and Vifor and royalties from UpToDate and Springer.
R.P.-F. has received research grants from Fresenius Medical Care and the National Council for Scientific and Technological Development; grants (paid to employer) from Akebia, AstraZeneca, Bayer, Boehringer Lilly and Novo Nordisk for participation in advisory boards and educational activities and is employed by Arbor Research Collaborative for Health, who runs the Dialysis Outcomes and Practice Patterns Study (DOPPS). Global support for the ongoing DOPPS programs is provided without restriction on publications by a variety of funders. Funding is provided to Arbor Research Collaborative for Health and not to R.P.-F. directly. For details, see
P.R. has received consultancy fees for Bayer, G3P, Idorsia and KBP; honoraria from Ablative Solutions, AstraZeneca, Bayer, Boehringer Ingelheim, CinCor, Corvidia, CVRx, Fresenius, Grünenthal, Novartis, Novo Nordisk, Roche, Sanofi, Sequana Medical, Servier, Stealth Peptides, Vifor Fresenius Medical Care Renal Pharma and Vifor Pharma, Inc.; personal fees from Ablative Solutions, Bayer, Boehringer Ingelheim, Corvidia, CVRx, Grünenthal, Idorsia, KBP, Novo Nordisk, Sanofi, Sequana Medical, Servier, Stealth Peptides and Vifor Pharma; grants and personal fees from AstraZeneca, Bayer, Fresenius, Novartis and Vifor Fresenius Medical Care Renal Pharma and nonfinancial support from Fresenius; has ownership interest in G3P and is cofounder of CardioRenal and has received research funding from Vifor Fresenius Medical Care Renal Pharma and Vifor Pharma.
B.P. has no financial disclosures.
E.B. is a member of the FIDELIO-DKD steering committee.
J.M. has received grants and/or honoraria for consultancy or lectures from Bayer, AstraZeneca, Astellas and Boehringer Ingelheim.
A.J. was previously a full-time employee of Bayer AG, Pharmaceuticals Division, Germany at the time of the studies and analysis. He is currently a full-time employee of Chiesi Farmaceutici S.p.A, Parma, Italy.
M.G., D.W. and R.L. are full-time employees of Bayer AG, Pharmaceuticals Division, Germany.
G.B. has received research funding, paid to the University of Chicago Medicine, from Bayer, Novo Nordisk and Vascular Dynamics during the conduct of the study; consultancy and personal fees from Alnylam, Merck and Relypsa; is editor of the
Figures
References
-
- Williams B, MacDonald TM, Morant Set al. Spironolactone versus placebo, bisoprolol, and doxazosin to determine the optimal treatment for drug-resistant hypertension (PATHWAY-2): a randomised, double-blind, crossover trial. Lancet 2015;386:2059–68. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(15)00257.... - PMC - PubMed
-
- Kidney Disease: Improving Global Outcomes . KDIGO 2021 clinical practice guideline for the management of blood pressure in chronic kidney disease. Kidney Int 2021;99(3 Suppl):S1–87.
Associated data
LinkOut - more resources
Full Text Sources
Medical
