

Measures of Admission Immunocoagulopathy as an Indicator for In-Hospital Mortality in Patients with Necrotizing Fasciitis: A Retrospective Study
- PMID: 36864907
- PMCID: PMC9974085
- DOI: 10.2106/JBJS.OA.22.00106
Measures of Admission Immunocoagulopathy as an Indicator for In-Hospital Mortality in Patients with Necrotizing Fasciitis: A Retrospective Study
Abstract
Necrotizing fasciitis is a rapidly progressive infection with a high mortality rate. Pathogens evade the host containment and bactericidal mechanisms by hijacking the coagulation and inflammation signaling pathways, leading to their rapid dissemination, thrombosis, organ dysfunction, and death. This study examines the hypothesis that measures of immunocoagulopathy upon admission could aid in the identification of patients with necrotizing fasciitis at high risk for in-hospital mortality.
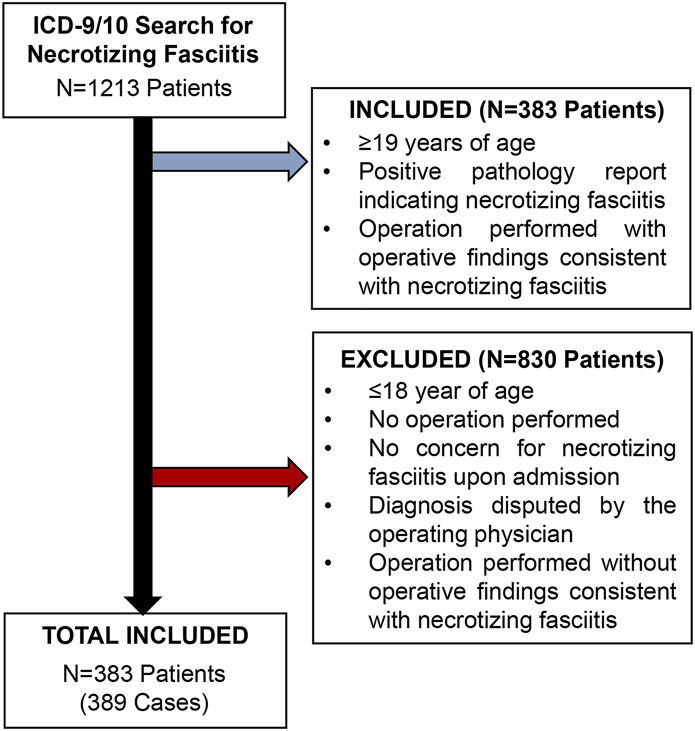
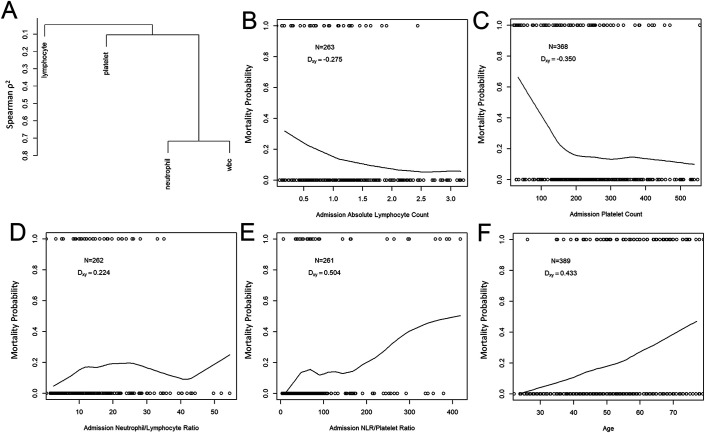
Methods: Demographic data, infection characteristics, and laboratory values from 389 confirmed necrotizing fasciitis cases from a single institution were analyzed. A multivariable logistic regression model was built on admission immunocoagulopathy measures (absolute neutrophil, absolute lymphocyte, and platelet counts) and patient age to predict in-hospital mortality.
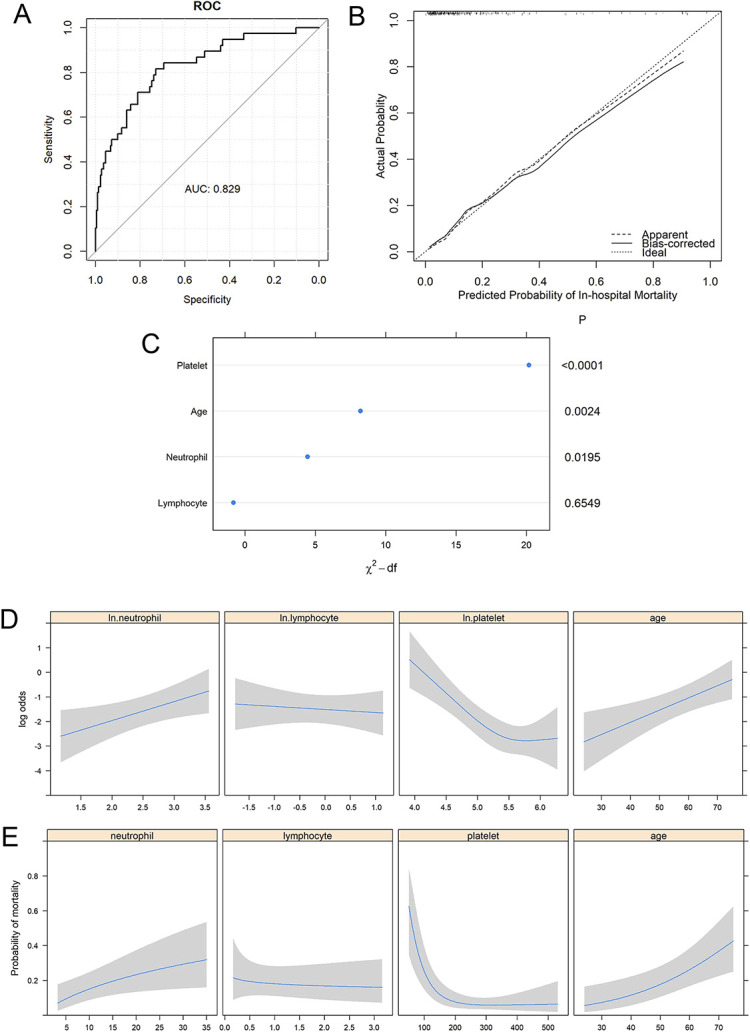
Results: The overall in-hospital mortality rate was 19.8% for the 389 cases and 14.6% for the 261 cases with complete measures of immunocoagulopathy on admission. A multivariable logistic regression model indicated that platelet count was the most important predictor of mortality, followed by age and absolute neutrophil count. Greater age, higher neutrophil count, and lower platelet count led to significantly higher risk of mortality. The model discriminated well between survivors and non-survivors, with an overfitting-corrected C-index of 0.806.
Conclusions: This study determined that measures of immunocoagulopathy and patient age at admission effectively prognosticated the in-hospital mortality risk of patients with necrotizing fasciitis. Given the accessibility of neutrophil-to-lymphocyte ratio and platelet count measurements determined from a simple complete blood-cell count with differential, future prospective studies examining the utility of these measures are warranted.
Level of evidence: Prognostic Level III. See Instructions for Authors for a complete description of levels of evidence.
Keywords: Acute phase response; immunocoagulopathy; in-hospital mortality; necrotizing fasciitis; neutrophil-to-lymphocyte ratio; orthopaedics.
Copyright © 2023 The Authors. Published by The Journal of Bone and Joint Surgery, Incorporated. All rights reserved.
Conflict of interest statement
Disclosure: The Disclosure of Potential Conflicts of Interest forms are provided with the online version of the article (http://links.lww.com/JBJSOA/A476).
Figures

References
-
- Benvenuti M, An T, Amaro E, Lovejoy S, Mencio G, Martus J, Mignemi M, Schoenecker JG. Double-edged sword: musculoskeletal infection provoked acute phase response in children. Orthop Clin North Am. 2017;48(2):181-97. - PubMed
-
- An TJ, Benvenuti MA, Mignemi ME, Thomsen IP, Schoenecker JG. Pediatric musculoskeletal infection: Hijacking the acute-phase response. JBJS Rev. 2016. Sep 27;4(9):e4. - PubMed
-
- Moore-Lotridge SN, Gibson BH, Duvernay MT, Martus JE, Thomsen IP, Schoenecker JG. Pediatric Musculoskeletal Infection. J Pediatric Orthopaedic Society North America. 2020;2(2).
-
- Kobayashi SD, Voyich JM, Burlak C, DeLeo FR. Neutrophils in the innate immune response. Arch Immunol Ther Exp (Warsz). 2005;53(6):505-517. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials