

Choosing the right treatment for the right lesion, part I: a narrative review of the role of plain balloon angioplasty in dialysis access maintenance
- PMID: 36864950
- PMCID: PMC9971312
- DOI: 10.21037/cdt-22-375
Choosing the right treatment for the right lesion, part I: a narrative review of the role of plain balloon angioplasty in dialysis access maintenance
Abstract
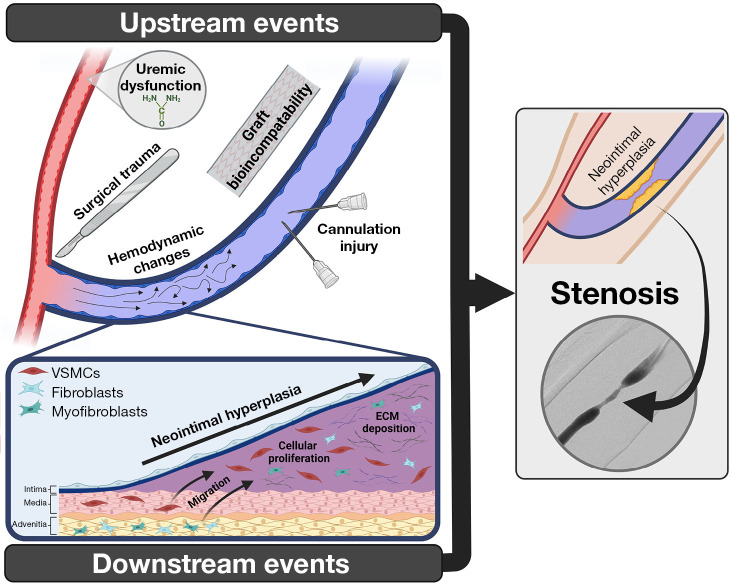
Background and objective: The majority of patients with end-stage renal disease (ESRD) requiring hemodialysis (HD) do so via an arteriovenous fistula (AVF) or graft. Both of these accesses are complicated by dysfunction related to neointimal hyperplasia (NIH) and subsequent stenosis. Percutaneous balloon angioplasty using plain balloons is the first line treatment for clinically-significant stenosis, with excellent initial response rates, however, with poor long-term patency and need for frequent reintervention. Recent research has sought to improve patency rates utilizing antiproliferative drug-coated balloons (DCBs), however, their role in treatment has not yet been fully determined. In part one of this two-part review, we aim to provide a comprehensive overview of the mechanisms of arteriovenous (AV) access stenosis, the evidence behind their treatment with high-quality plain balloon angioplasty techniques, and treatment considerations for specific stenotic lesions.
Methods: An electronic search was performed on PubMed and EMBASE to identify relevant articles from 1980 to 2022. The highest available level of evidence regarding stenosis pathophysiology, angioplasty techniques, and approaches to treating different types of lesions within fistulas and grafts were included as part of this narrative review.
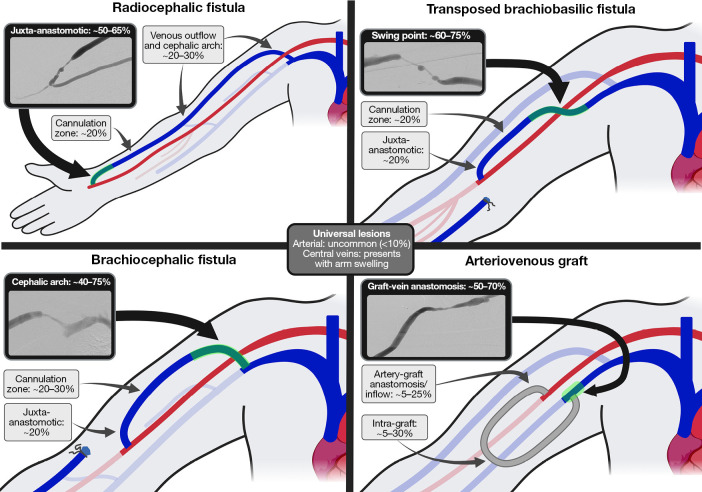
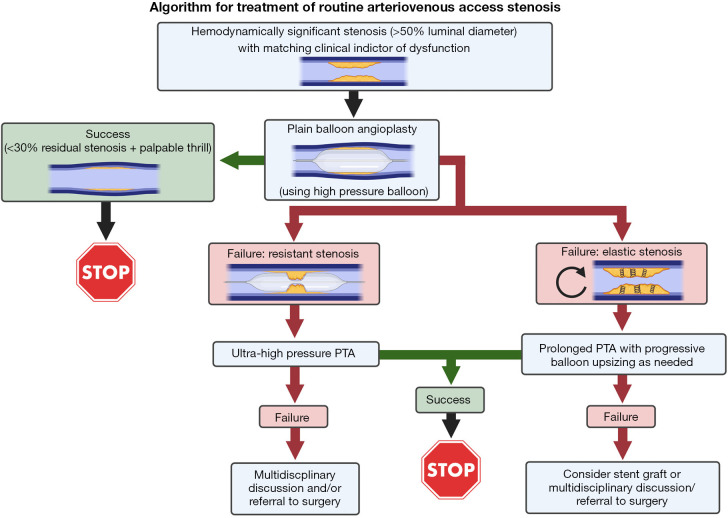
Key content and findings: NIH, and subsequent stenoses, develop via a combination of upstream events, causing vascular damage, and downstream events, representing the subsequent biologic response. The large majority of stenotic lesions can be treated utilizing high-pressure balloon angioplasty, with the addition of ultra-high pressure balloon (UHPB) angioplasty for resistant lesions and prolonged angioplasty with progressive balloon upsizing for elastic lesions. Additional treatment considerations must be taken into account when treating specific lesions, including cephalic arch and swing point stenoses in fistulas and graft-vein anastomotic stenoses in grafts, amongst others.
Conclusions: High-quality plain balloon angioplasty, performed utilizing the available evidence-basis regarding technique and considerations for specific lesion locations, is successful in treating the large majority of AV access stenoses. While initially successful, patency rates remain non-durable. Part two of this review will discuss the evolving role of DCBs, which seek to improve angioplasty outcomes.
Keywords: Hemodialysis (HD); angioplasty; fistula; graft; stenosis.
2023 Cardiovascular Diagnosis and Therapy. All rights reserved.
Conflict of interest statement
Conflicts of Interest: Both authors have completed the ICMJE uniform disclosure form (available at https://cdt.amegroups.com/article/view/10.21037/cdt-22-375/coif). The series “Endovascular and Surgical Interventions in the End Stage Renal Disease Population” was commissioned by the editorial office without any funding or sponsorship. SOT has received consultant fees from Medcomp, BD, and Cook and royalty fees from Teleflex. The authors have no other conflicts of interest to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources