

Neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios: associations with mortality in a haemodialysis cohort
- PMID: 36865003
- PMCID: PMC9972818
- DOI: 10.1093/ckj/sfac248
Neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios: associations with mortality in a haemodialysis cohort
Abstract
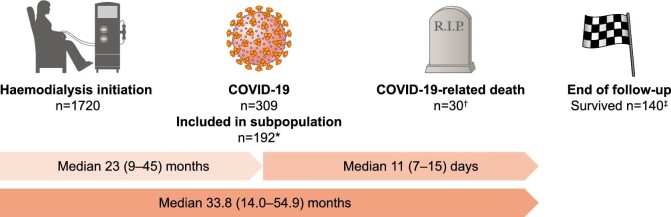
Background: Lymphocyte ratios reflect inflammation and have been associated with adverse outcomes in a range of diseases. We sought to determine any association between neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) and mortality in a haemodialysis cohort, including a coronavirus disease 2019 (COVID-19) infection subpopulation.
Methods: A retrospective analysis was performed of adults commencing hospital haemodialysis in the West of Scotland during 2010-21. NLR and PLR were calculated from routine samples around haemodialysis initiation. Kaplan-Meier and Cox proportional hazards analyses were used to assess mortality associations.
Results: In 1720 haemodialysis patients over a median of 21.9 (interquartile range 9.1-42.9) months, there were 840 all-cause deaths. NLR but not PLR was associated with all-cause mortality after multivariable adjustment [adjusted hazard ratio (aHR) for in participants with baseline NLR in quartile 4 (NLR ≥8.23) versus quartile 1 (NLR <3.12) 1.63, 95% confidence interval (CI) 1.32-2.00]. The association was stronger for cardiovascular death (NLR quartile 4 versus 1 aHR 3.06, 95% CI 1.53-6.09) than for non-cardiovascular death (NLR quartile 4 versus 1 aHR 1.85, 95% CI 1.34-2.56). In the COVID-19 subpopulation, both NLR and PLR at haemodialysis initiation were associated with risk of COVID-19-related death after adjustment for age and sex (NLR: aHR 4.69, 95% CI 1.48-14.92 and PLR: aHR 3.40, 95% CI 1.02-11.36; for highest vs lowest quartiles).
Conclusions: NLR is strongly associated with mortality in haemodialysis patients while the association between PLR and adverse outcomes is weaker. NLR is an inexpensive, readily available biomarker with potential utility in risk stratification of haemodialysis patients.
Keywords: COVID-19; haemodialysis; inflammation; lymphocyte; mortality.
© The Author(s) 2022. Published by Oxford University Press on behalf of the ERA.
Figures



References
Grants and funding
LinkOut - more resources
Full Text Sources
