

Trends in LDL-C following coronary angiography involving assessment by fractional flow reserve in obstructive vs non-obstructive coronary artery disease
- PMID: 36865903
- PMCID: PMC9971059
- DOI: 10.1016/j.ajpc.2023.100473
Trends in LDL-C following coronary angiography involving assessment by fractional flow reserve in obstructive vs non-obstructive coronary artery disease
Abstract
Background: We sought to determine whether management of LDL-C following invasive angiography and assessment by fractional flow reserve (FFR) differs between those with obstructive vs non-obstructive CAD.
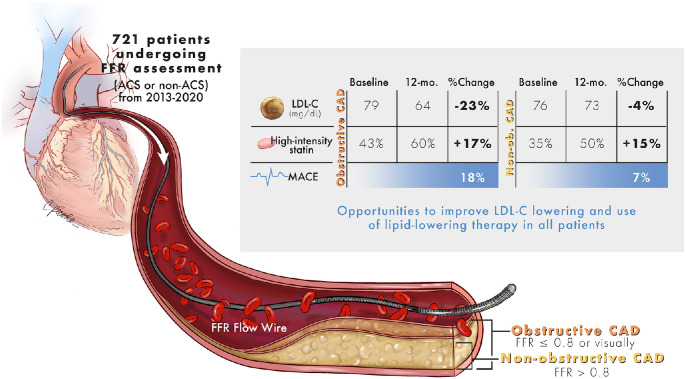
Methods: Retrospective study of 721 patients undergoing coronary angiography involving assessment by FFR between 2013 and 2020 at a single academic center. Groups with obstructive vs non-obstructive CAD by index angiographic and FFR findings were compared over 1 year of follow-up.
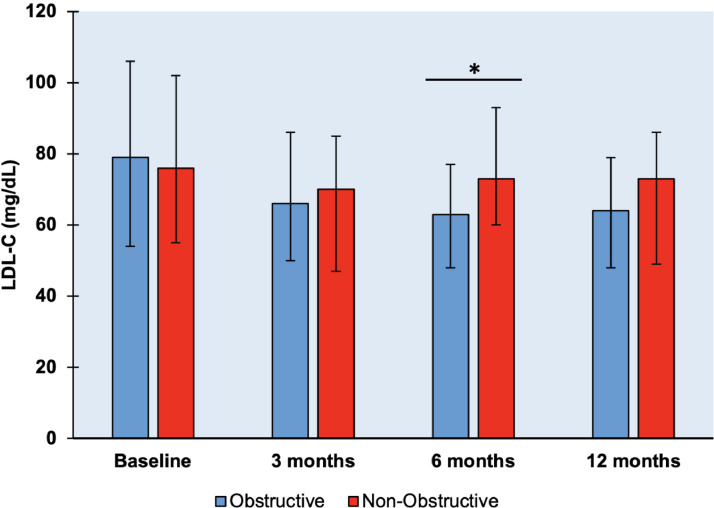
Results: Based on index angiographic and FFR findings, 421 (58%) patients had obstructive CAD vs 300 (42%) with non-obstructive CAD, mean (±SD) age 66±11 years, 217 (30%) women, and 594 (82%) white. There was no difference in baseline LDL-C. At 3-months follow-up, LDL-C was lower than baseline in both groups, with no between group difference. In contrast, at 6-months, median (Q1, Q3) LDL-C was significantly higher in non-obstructive vs obstructive CAD (LDL-C 73 (60, 93) vs 63 (48, 77) mg/dL, respectively (p = 0.003), (p = 0.001 in multivariable linear regression)). At 12-months, LDL-C remained higher in non-obstructive vs obstructive CAD (LDL-C 73 (49, 86) vs 64 (48, 79) mg/dL, respectively, although not statistically significant (p = 0.104)). The rate of high-intensity statin use was lower among those with non-obstructive CAD vs obstructive CAD at all time points (p < 0.05).
Conclusions: After coronary angiography involving FFR, there is intensification of LDL-C lowering at 3-months follow-up in both obstructive and non-obstructive CAD. However, by 6-months follow-up LDL-C is significantly higher among those with non-obstructive CAD vs obstructive CAD. Following coronary angiography involving FFR, patients with non-obstructive CAD may benefit from greater attention to LDL-C lowering to reduce residual ASCVD risk.
Keywords: Coronary angiography; Coronary artery disease; Dyslipidemia; Fractional flow reserve.
© 2023 The Authors. Published by Elsevier B.V.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Clinical outcomes of fractional flow reserve by computed tomographic angiography-guided diagnostic strategies vs. usual care in patients with suspected coronary artery disease: the prospective longitudinal trial of FFR(CT): outcome and resource impacts study.Eur Heart J. 2015 Dec 14;36(47):3359-67. doi: 10.1093/eurheartj/ehv444. Epub 2015 Sep 1. Eur Heart J. 2015. PMID: 26330417 Free PMC article.
-
Effect of Atorvastatin on Serial Changes in Coronary Physiology and Plaque Parameters.JACC Asia. 2022 Nov 1;2(6):691-703. doi: 10.1016/j.jacasi.2022.07.010. eCollection 2022 Nov. JACC Asia. 2022. PMID: 36444331 Free PMC article.
-
Impact of machine-learning CT-derived fractional flow reserve for the diagnosis and management of coronary artery disease in the randomized CRESCENT trials.Eur Radiol. 2020 Jul;30(7):3692-3701. doi: 10.1007/s00330-020-06778-w. Epub 2020 Mar 12. Eur Radiol. 2020. PMID: 32166492 Free PMC article.
-
Meta-Analysis of Diagnostic Performance of Coronary Computed Tomography Angiography, Computed Tomography Perfusion, and Computed Tomography-Fractional Flow Reserve in Functional Myocardial Ischemia Assessment Versus Invasive Fractional Flow Reserve.Am J Cardiol. 2015 Nov 1;116(9):1469-78. doi: 10.1016/j.amjcard.2015.07.078. Epub 2015 Aug 14. Am J Cardiol. 2015. PMID: 26347004 Free PMC article. Review.
-
Fractional flow reserve versus angiography alone in guiding myocardial revascularisation: a systematic review and meta-analysis of randomised trials.Heart. 2022 Oct 13;108(21):1699-1706. doi: 10.1136/heartjnl-2021-320768. Heart. 2022. PMID: 35568392
References
-
- Lawton J.S., Tamis-Holland J.E., Bangalore S., Bates E.R., Beckie T.M., Bischoff J.M., et al. 2021 acc/aha/scai guideline for coronary artery revascularization: a report of the american college of cardiology/american heart association joint committee on clinical practice guidelines. Circulation. 2022;145:e18–e114. - PubMed
-
- Chow B.J., Small G., Yam Y., Chen L., McPherson R., Achenbach S., et al. Prognostic and therapeutic implications of statin and aspirin therapy in individuals with nonobstructive coronary artery disease: results from the confirm (coronary CT angiography evaluation for clinical outcomes: an international multicenter registry) registry. Arterioscler Thromb Vasc Biol. 2015;35:981–989. - PMC - PubMed
-
- Falk E., Shah P.K., Fuster V. Coronary plaque disruption. Circulation. 1995;92:657–671. - PubMed
-
- Xaplanteris P., Fournier S., Pijls N.H.J., Fearon W.F., Barbato E., Tonino P.A.L., et al. Five-year outcomes with PCI guided by fractional flow reserve. N Engl J Med. 2018;379:250–259. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
