

Chinese herbal medicine for threatened miscarriage: An updated systematic review and meta-analysis
- PMID: 36865912
- PMCID: PMC9971626
- DOI: 10.3389/fphar.2023.1083746
Chinese herbal medicine for threatened miscarriage: An updated systematic review and meta-analysis
Abstract
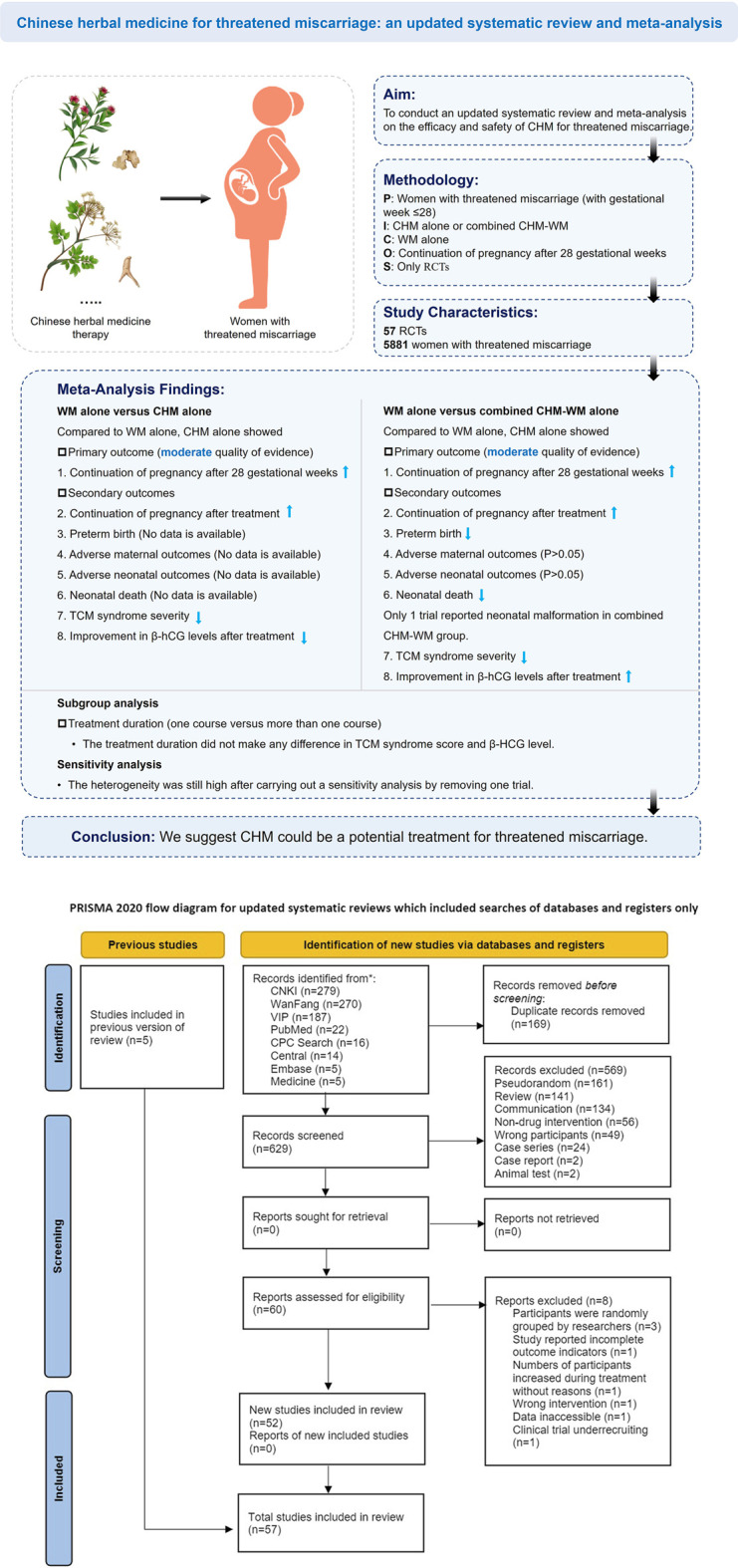
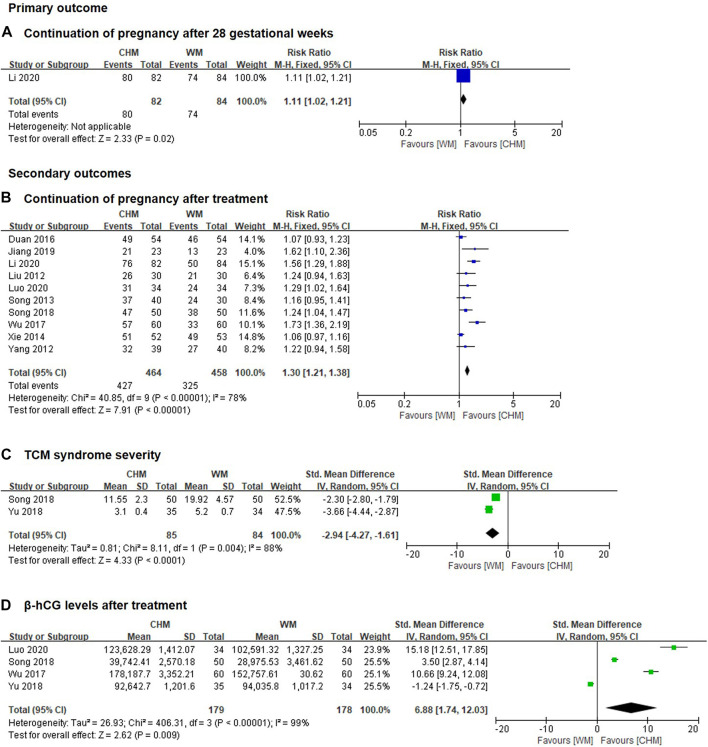
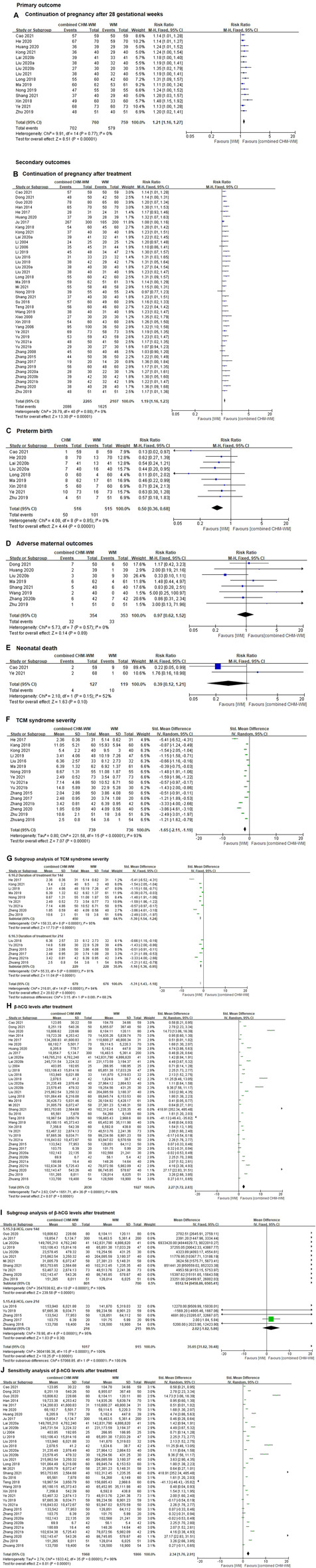
Objective: To conduct an updated systematic review and meta-analysis on the efficacy and safety of Chinese herbal medicine (CHM) for threatened miscarriage. Data Sources: Electronic databases were searched from inception to 30 June 2022. Study Eligibility Criteria: Only randomized controlled trials (RCTs) that assessed the efficacy and safety of CHM or combined CHM and Western medicine (CHM-WM) and compared with other treatments for threatened miscarriage were included for analysis. Methods: Three review authors independently evaluated included studies, assessed the risk of bias and extracted data for meta-analysis (continuation of pregnancy after 28 gestational weeks, continuation of pregnancy after treatment, preterm birth, adverse maternal outcomes, neonatal death, TCM syndrome severity, β-hCG levels after treatment), sensitivity analysis (β-hCG level) and subgroup analysis (TCM syndrome severity, β-hCG level). The risk ratio and 95% confidence interval were calculated by RevMan. Certainty of the evidence was assessed according to GRADE. Results: Overall, 57 RCTs involving 5,881 patients met the inclusion criteria. Compared with WM alone, CHM alone showed significant higher incidence of continuation of pregnancy after 28 gestational weeks (Risk Ratio (RR) 1.11; 95% CI 1.02 to 1.21; n = 1; moderate quality of evidence), continuation of pregnancy after treatment (RR 1.30; 95% CI 1.21 to 1.38; n = 10; moderate quality of evidence), higher β-hCG level (Standardized Mean Difference (SMD) 6.88; 95% CI 1.74 to 12.03; n = 4) and lower Traditional Chinese medicine (TCM) syndrome severity (SMD -2.94; 95% CI -4.27 to -1.61; n = 2). Compared with WM alone, combined CHM-WM showed significant higher incidence of continuation of pregnancy after 28 gestational weeks (RR 1.21; 95% CI 1.16 to 1.27; n = 15; moderate quality of evidence), continuation of pregnancy after treatment (RR 1.19; 95% CI 1.16 to 1.23; n = 41; moderate quality of evidence), higher β-hCG level (SMD 2.27; 95% CI 1.72 to 2.83; n = 37) and lower TCM syndrome severity (SMD -1.74; 95% CI -2.21 to -1.27; n = 15). No significant differences in reducing the adverse maternal outcomes and neonatal death were found in combined CHM-WM compared with WM alone (RR 0.97; 95% CI 0.62 to 1.52; n = 8; RR 0.39; 95% CI 0.12 to 1.21; n = 2). Conclusion: Current evidence supported CHM could be a potential treatment for threatened miscarriage. However, results should be interpreted with caution considering the low to moderate quality of the available evidence. Systematic Review Registration: [https://inplasy.com/inplasy-2022-6-0107/], identifier [INPLASY20220107].
Keywords: Chinese herbal medicine; efficacy; meta-analysis; safety; systematic review; threatened miscarriage.
Copyright © 2023 Xie, Zhang, Mou, He, Li, Wang, Fan and Li.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
The efficacy and safety of Chinese herbal medicine as an add-on therapy for type 2 diabetes mellitus patients with carotid atherosclerosis: An updated meta-analysis of 27 randomized controlled trials.Front Pharmacol. 2023 Mar 23;14:1091718. doi: 10.3389/fphar.2023.1091718. eCollection 2023. Front Pharmacol. 2023. PMID: 37033624 Free PMC article.
-
Efficacy and safety of Gushen Antai Pills combined with dydrogesterone in the treatment of threatened miscarriage: a systematic review and meta-analysis.Front Pharmacol. 2023 Jun 2;14:1138968. doi: 10.3389/fphar.2023.1138968. eCollection 2023. Front Pharmacol. 2023. PMID: 37332346 Free PMC article.
-
Efficacy of Chinese herbal medicine on nasal itching in children with allergic rhinitis: a systematic review and meta-analysis.Front Pharmacol. 2023 Aug 23;14:1240917. doi: 10.3389/fphar.2023.1240917. eCollection 2023. Front Pharmacol. 2023. PMID: 37680707 Free PMC article.
-
The efficacy and safety of combined chinese herbal medicine and western medicine therapy for COVID-19: a systematic review and meta-analysis.Chin Med. 2022 Jun 21;17(1):77. doi: 10.1186/s13020-022-00600-z. Chin Med. 2022. PMID: 35729581 Free PMC article. Review.
-
Integrated Chinese herbal medicine with Western Medicine versus Western Medicine in the effectiveness of primary hypertension treatment: A systematic review and meta-analysis of randomized controlled trials.J Ethnopharmacol. 2023 Jan 10;300:115703. doi: 10.1016/j.jep.2022.115703. Epub 2022 Sep 10. J Ethnopharmacol. 2023. PMID: 36096347
Cited by
-
Predictors of pregnant and breastfeeding women's intention to use traditional Chinese medicine: a cross-sectional study from China.BMC Complement Med Ther. 2025 Jun 3;25(1):199. doi: 10.1186/s12906-025-04952-5. BMC Complement Med Ther. 2025. PMID: 40462139 Free PMC article.
-
Progestogen therapy in threatened miscarriage and unexplained recurrent pregnancy loss: Recommendations by the Thai interest group.J Obstet Gynaecol Res. 2025 Aug;51(8):e70038. doi: 10.1111/jog.70038. J Obstet Gynaecol Res. 2025. PMID: 40797287 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous