

Effects of peripheral active warming and passive insulation on core body temperature during feline ovariohysterectomy: a multi-arm randomized clinical trial
- PMID: 36867072
- PMCID: PMC10812009
- DOI: 10.1177/1098612X231157585
Effects of peripheral active warming and passive insulation on core body temperature during feline ovariohysterectomy: a multi-arm randomized clinical trial
Abstract
Objectives: Hypothermia is a common complication of anesthesia, particularly in cats. Some veterinarians insulate the extremities of cats as a preventive measure, and there is evidence that heating the extremities of dogs decreases the rate of heat loss from the core. This study investigated whether active warming or passive insulation of the extremities of cats resulted in a slower decrease in rectal temperature during anesthesia.
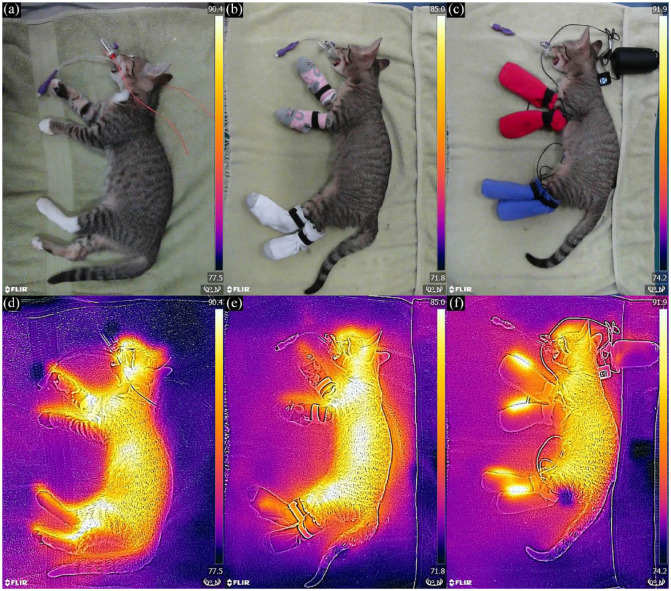
Methods: Female cats were assigned via block randomization to passive (cotton toddler socks), active (heated toddler socks) or control group (uncovered extremities). Rectal temperature was monitored every 5 mins from induction through return to trap/carrier (final temperature). Multivariable linear regression models were used to compare temperature (rate change and final) between groups.
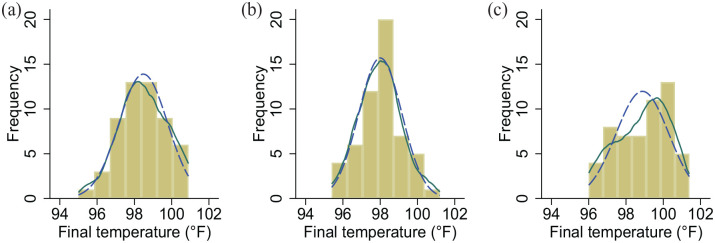
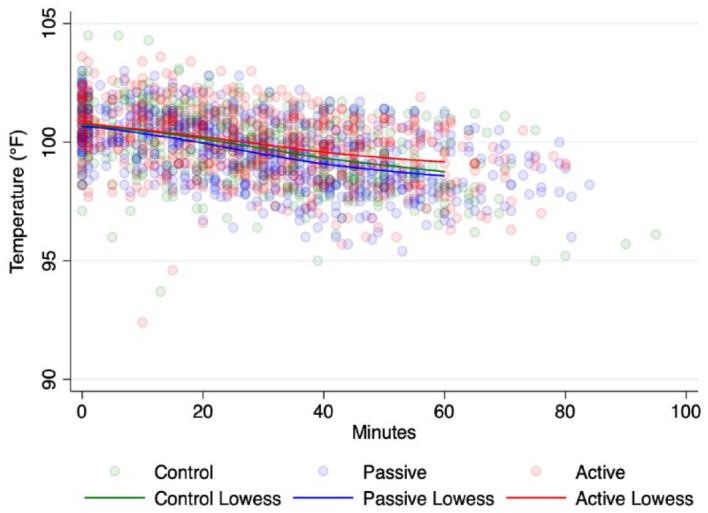
Results: There were 164 cats with 1757 temperature readings. Mean total duration of anesthesia was 53 ± 13 mins. The temperature of all groups decreased linearly over time (all P <0.0001), with the rates of temperature decrease being -0.039°F/min (95% confidence interval [CI] -0.043 to -0.035)/-0.022°C (95% CI -0.024 to -0.019), -0.039°F/min (95% CI -0.042 to -0.035)/-0.022°C (95% CI -0.023 to -0.019) and -0.029°F/min (95% CI -0.032 to -0.025)/-0.016°C (95% CI -0.018 to -0.014) for the control, passive and active groups, respectively. The control, passive and active groups had median final temperatures of 98.4°F (interquartile range [IQR] 97.6-99.4)/36.9°C (IQR 36.4-37.4), 98.0°F (IQR 97.2-98.7)/36.7°C (IQR 36.2-37.1) and 99.1°F (IQR 97.7-100.0)/37.3°C (IQR 36.5-37.8), respectively. After controlling for weight, postinduction temperature and duration of anesthesia, and as compared with controls, the final temperature of the active group was predicted to be 0.54°F (95% CI 0.03-1.01)/0.3°C (95% CI 0.02-0.56) greater (P = 0.023), while the passive group was not significantly different (P = 0.130).
Conclusions and relevance: The rate of rectal temperature decrease was significantly slower for the active group compared with the other groups. Although the cumulative difference in final temperature reading was modest, superior materials might enhance performance. Cotton toddler socks alone did not slow the rate of temperature decrease.
Keywords: Anesthesia; anaesthesia; high-quality high-volume spay–neuter; hypothermia; shelter medicine; surgery; trap–neuter–vaccinate–return.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Pottie RG, Dart CM, Perkins NR, et al. Effect of hypothermia on recovery from general anaesthesia in the dog. Aust Vet J 2007; 85: 158–162. - PubMed
-
- Sessler DI. Mild perioperative hypothermia. N Engl J Med 1997; 336: 1730–1737. - PubMed
-
- Reynolds L, Beckmann J, Kurz A. Perioperative complications of hypothermia. Best Pract Res Clin Anaesthesiol 2008; 22: 645–657. - PubMed
-
- Öner Cengiz H, Uçar S, Yilmaz M. The role of perioperative hypothermia in the development of surgical site infection: a systematic review. AORN J 2021; 113: 265–275. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
