

Antidepressant Augmentation versus Switch in Treatment-Resistant Geriatric Depression
- PMID: 36867173
- PMCID: PMC10568698
- DOI: 10.1056/NEJMoa2204462
Antidepressant Augmentation versus Switch in Treatment-Resistant Geriatric Depression
Abstract
Background: The benefits and risks of augmenting or switching antidepressants in older adults with treatment-resistant depression have not been extensively studied.
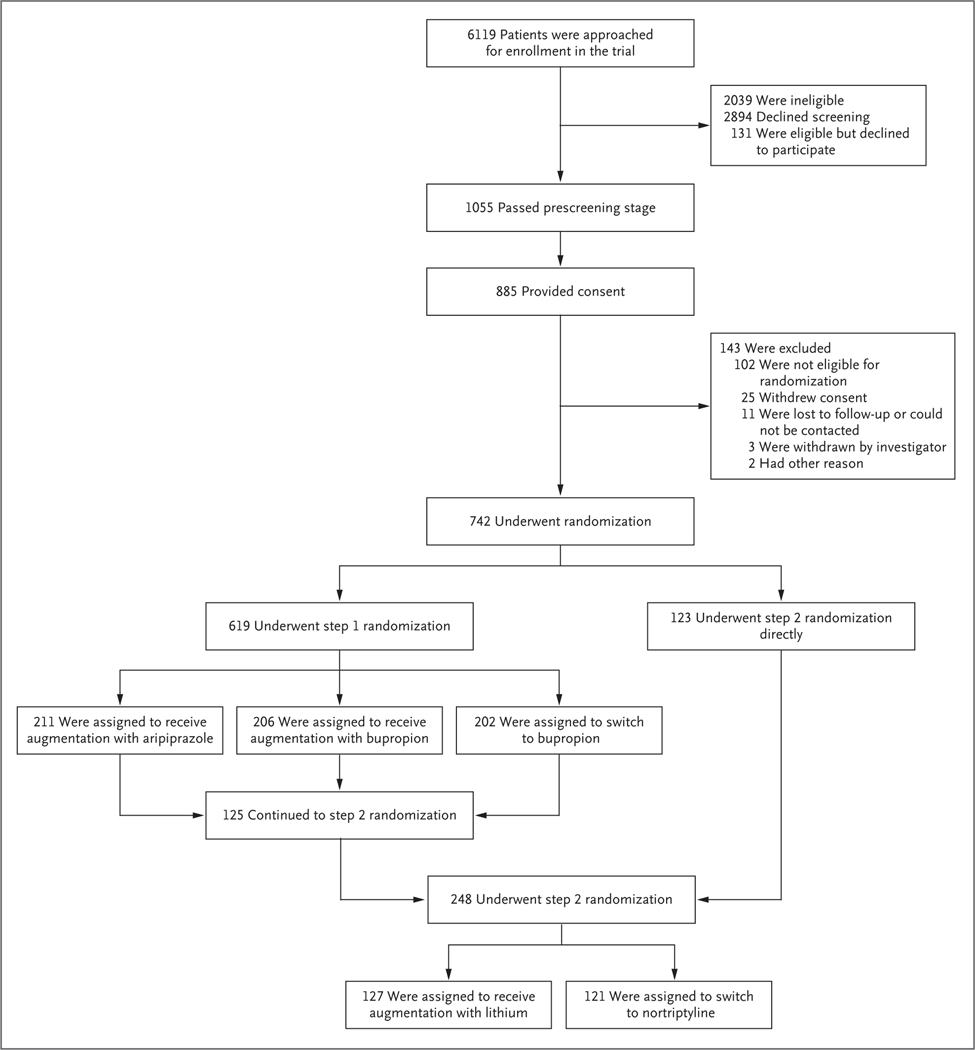
Methods: We conducted a two-step, open-label trial involving adults 60 years of age or older with treatment-resistant depression. In step 1, patients were randomly assigned in a 1:1:1 ratio to augmentation of existing antidepressant medication with aripiprazole, augmentation with bupropion, or a switch from existing antidepressant medication to bupropion. Patients who did not benefit from or were ineligible for step 1 were randomly assigned in step 2 in a 1:1 ratio to augmentation with lithium or a switch to nortriptyline. Each step lasted approximately 10 weeks. The primary outcome was the change from baseline in psychological well-being, assessed with the National Institutes of Health Toolbox Positive Affect and General Life Satisfaction subscales (population mean, 50; higher scores indicate greater well-being). A secondary outcome was remission of depression.
Results: In step 1, a total of 619 patients were enrolled; 211 were assigned to aripiprazole augmentation, 206 to bupropion augmentation, and 202 to a switch to bupropion. Well-being scores improved by 4.83 points, 4.33 points, and 2.04 points, respectively. The difference between the aripiprazole-augmentation group and the switch-to-bupropion group was 2.79 points (95% CI, 0.56 to 5.02; P = 0.014, with a prespecified threshold P value of 0.017); the between-group differences were not significant for aripiprazole augmentation versus bupropion augmentation or for bupropion augmentation versus a switch to bupropion. Remission occurred in 28.9% of patients in the aripiprazole-augmentation group, 28.2% in the bupropion-augmentation group, and 19.3% in the switch-to-bupropion group. The rate of falls was highest with bupropion augmentation. In step 2, a total of 248 patients were enrolled; 127 were assigned to lithium augmentation and 121 to a switch to nortriptyline. Well-being scores improved by 3.17 points and 2.18 points, respectively (difference, 0.99; 95% CI, -1.92 to 3.91). Remission occurred in 18.9% of patients in the lithium-augmentation group and 21.5% in the switch-to-nortriptyline group; rates of falling were similar in the two groups.
Conclusions: In older adults with treatment-resistant depression, augmentation of existing antidepressants with aripiprazole improved well-being significantly more over 10 weeks than a switch to bupropion and was associated with a numerically higher incidence of remission. Among patients in whom augmentation or a switch to bupropion failed, changes in well-being and the occurrence of remission with lithium augmentation or a switch to nortriptyline were similar. (Funded by the Patient-Centered Outcomes Research Institute; OPTIMUM ClinicalTrials.gov number, NCT02960763.).
Copyright © 2023 Massachusetts Medical Society.
Figures
Comment in
-
Antidepressant Augmentation versus Switch in Treatment-Resistant Geriatric Depression.N Engl J Med. 2023 May 25;388(21):2012. doi: 10.1056/NEJMc2304804. N Engl J Med. 2023. PMID: 37224207 No abstract available.
-
Antidepressant Augmentation versus Switch in Treatment-Resistant Geriatric Depression.N Engl J Med. 2023 May 25;388(21):2012-2013. doi: 10.1056/NEJMc2304804. N Engl J Med. 2023. PMID: 37224208 No abstract available.
-
Antidepressant Augmentation versus Switch in Treatment-Resistant Geriatric Depression. Reply.N Engl J Med. 2023 May 25;388(21):2013. doi: 10.1056/NEJMc2304804. N Engl J Med. 2023. PMID: 37224209 No abstract available.
References
-
- Mojtabai R Diagnosing depression in older adults in primary care. N Engl J Med 2014; 370: 1180–2. - PubMed
-
- Hamm ME, Karp JF, Lenard E, et al. “What else can we do?” — provider perspectives on treatment-resistant depression in late life. J Am Geriatr Soc 2022; 70: 1190–7. - PubMed
-
- Berlim MT, Turecki G. What is the meaning of treatment resistant/refractory major depression (TRD)? A systematic review of current randomized trials. Eur Neuropsychopharmacol 2007; 17:696–707. - PubMed
-
- Beekman AT, Penninx BW, Deeg DJ, de Beurs E, Geerling SW, van Tilburg W. The impact of depression on the well-being, disability and use of services in older adults: a longitudinal perspective. Acta Psychiatr Scand 2002; 105: 20–7. - PubMed
-
- Lenze EJ, Rogers JC, Martire LM, et al. The association of late-life depression and anxiety with physical disability: a review of the literature and prospectus for future research. Am J Geriatr Psychiatry 2001; 9: 113–35. - PubMed