

Liquid biopsy-based protein biomarkers for risk prediction, early diagnosis, and prognostication of cholangiocarcinoma
- PMID: 36868481
- PMCID: PMC10292605
- DOI: 10.1016/j.jhep.2023.02.027
Liquid biopsy-based protein biomarkers for risk prediction, early diagnosis, and prognostication of cholangiocarcinoma
Abstract
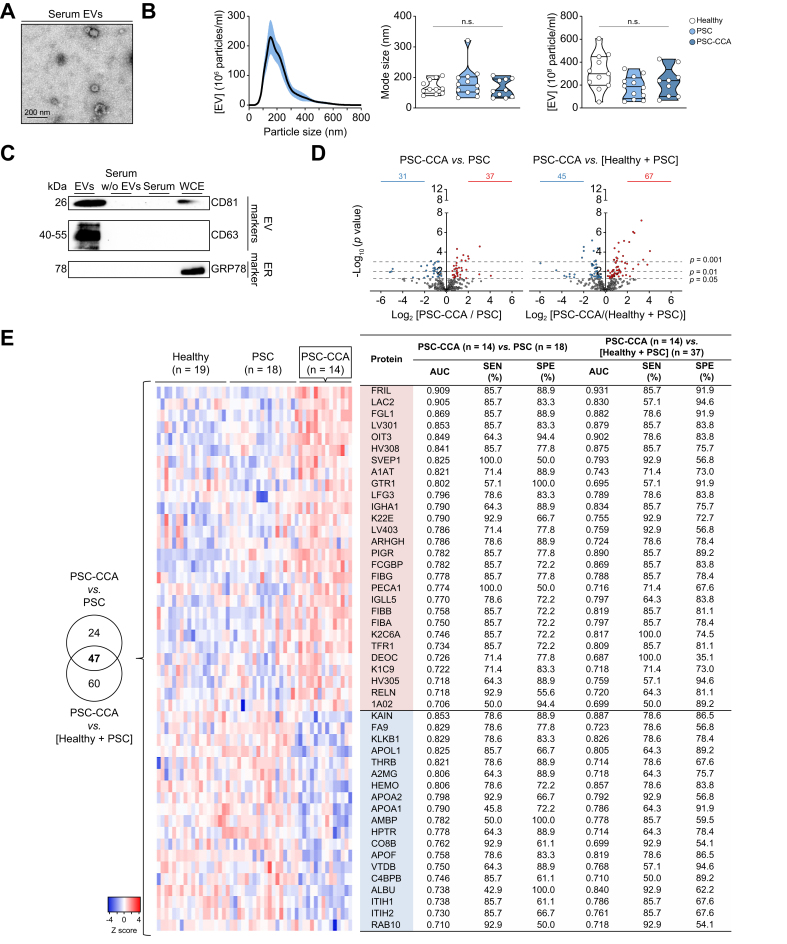
Background & aims: Cholangiocarcinoma (CCA), heterogeneous biliary tumours with dismal prognosis, lacks accurate early diagnostic methods especially important for individuals at high-risk (i.e. those with primary sclerosing cholangitis [PSC]). Here, we searched for protein biomarkers in serum extracellular vesicles (EVs).
Methods: EVs from patients with isolated PSC (n = 45), concomitant PSC-CCA (n = 44), PSC who developed CCA during follow-up (PSC to CCA; n = 25), CCAs from non-PSC aetiology (n = 56), and hepatocellular carcinoma (n = 34) and healthy individuals (n = 56) were characterised by mass spectrometry. Diagnostic biomarkers for PSC-CCA, non-PSC CCA, or CCAs regardless of aetiology (Pan-CCAs) were defined and validated by ELISA. Their expression was evaluated in CCA tumours at a single-cell level. Prognostic EV biomarkers for CCA were investigated.
Results: High-throughput proteomics of EVs identified diagnostic biomarkers for PSC-CCA, non-PSC CCA, or Pan-CCA, and for the differential diagnosis of intrahepatic CCA and hepatocellular carcinoma, which were cross-validated by ELISA using total serum. Machine learning-based algorithms disclosed CRP/FIBRINOGEN/FRIL for the diagnosis of PSC-CCA (local disease [LD]) vs. isolated PSC (AUC = 0.947; odds ratio [OR] =36.9) and, combined with carbohydrate antigen 19-9, overpowers carbohydrate antigen 19-9 alone. CRP/PIGR/VWF allowed the diagnosis of LD non-PSC CCAs vs. healthy individuals (AUC = 0.992; OR = 387.5). It is noteworthy that CRP/FRIL accurately diagnosed LD Pan-CCA (AUC = 0.941; OR = 89.4). Levels of CRP/FIBRINOGEN/FRIL/PIGR showed predictive capacity for CCA development in PSC before clinical evidence of malignancy. Multi-organ transcriptomic analysis revealed that serum EV biomarkers were mostly expressed in hepatobiliary tissues, and single-cell RNA sequencing and immunofluorescence analysis of CCA tumours showed their presence mainly in malignant cholangiocytes. Multivariable analysis unveiled EV prognostic biomarkers, with COMP/GNAI2/CFAI and ACTN1/MYCT1/PF4V associated negatively and positively with patients' survival, respectively.
Conclusions: Serum EVs contain protein biomarkers for the prediction, early diagnosis, and prognostication of CCA that are detectable using total serum, representing a tumour cell-derived liquid biopsy tool for personalised medicine.
Impact and implications: The accuracy of current imaging tests and circulating tumour biomarkers for cholangiocarcinoma (CCA) diagnosis is far from satisfactory. Most CCAs are considered sporadic, although up to 20% of patients with primary sclerosing cholangitis (PSC) develop CCA during their lifetime, constituting a major cause of PSC-related death. This international study has proposed protein-based and aetiology-related logistic models with predictive, diagnostic, or prognostic capacities by combining two to four circulating protein biomarkers, moving a step forward into personalised medicine. These novel liquid biopsy tools may allow the (i) easy and non-invasive diagnosis of sporadic CCAs, (ii) identification of patients with PSC with higher risk for CCA development, (iii) establishment of cost-effective surveillance programmes for the early detection of CCA in high-risk populations (e.g. PSC), and (iv) prognostic stratification of patients with CCA, which, altogether, may increase the number of cases eligible for potentially curative options or to receive more successful treatments, decreasing CCA-related mortality.
Keywords: Cholangiocarcinoma; Extracellular vesicles; Liquid biopsy; Mass spectrometry; Primary sclerosing cholangitis; Protein biomarkers; Single-cell RNA-sequencing.
Copyright © 2023 The Authors. Published by Elsevier B.V. All rights reserved.
Figures








References
-
- Rodrigues P.M., Olaizola P., Paiva N.A., Olaizola I., Agirre-Lizaso A., Landa A., et al. Pathogenesis of cholangiocarcinoma. Annu Rev Pathol. 2021;16:433–463. - PubMed
-
- Izquierdo-Sanchez L., Lamarca A., La Casta A., Buettner S., Utpatel K., Klumpen H.J., et al. Cholangiocarcinoma landscape in Europe: diagnostic, prognostic and therapeutic insights from the ENSCCA Registry. J Hepatol. 2022;76:1109–1121. - PubMed
-
- Macias R.I.R., Cardinale V., Kendall T.J., Avila M.A., Guido M., Coulouarn C., et al. Clinical relevance of biomarkers in cholangiocarcinoma: critical revision and future directions. Gut. 2022;71:1669–1683. - PubMed
-
- Valle J.W., Borbath I., Khan S.A., Huguet F., Gruenberger T., Arnold D., et al. Biliary cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2016;27:v28–v37. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
