

Critical Closing Pressure and Cerebrovascular Resistance Responses to Intracranial Pressure Variations in Neurocritical Patients
- PMID: 36869208
- PMCID: PMC10541829
- DOI: 10.1007/s12028-023-01691-8
Critical Closing Pressure and Cerebrovascular Resistance Responses to Intracranial Pressure Variations in Neurocritical Patients
Abstract
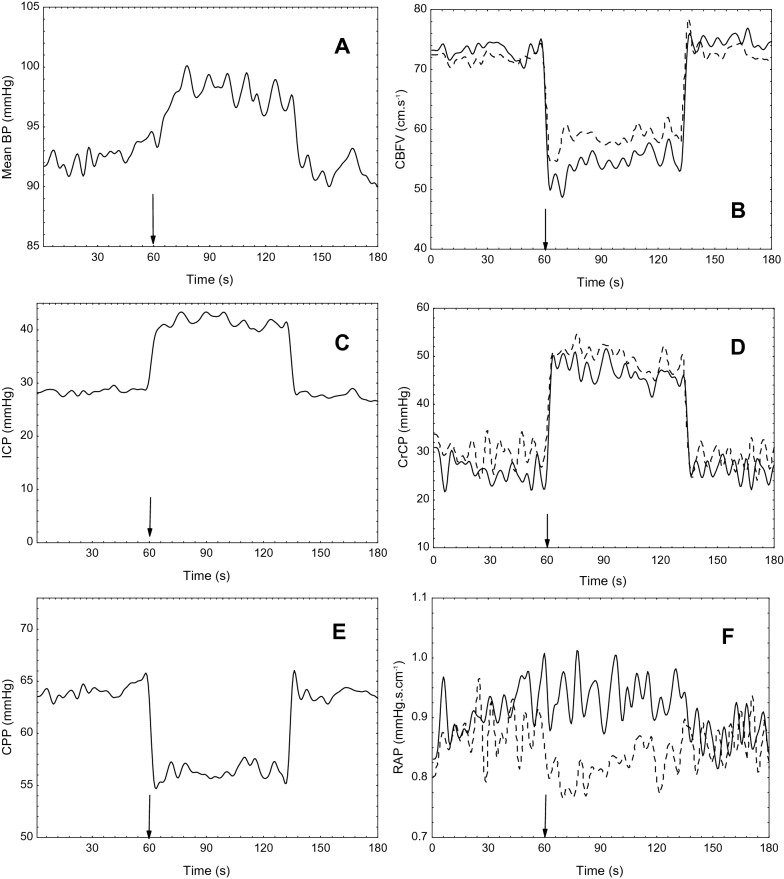
Background: Critical closing pressure (CrCP) and resistance-area product (RAP) have been conceived as compasses to optimize cerebral perfusion pressure (CPP) and monitor cerebrovascular resistance, respectively. However, for patients with acute brain injury (ABI), the impact of intracranial pressure (ICP) variability on these variables is poorly understood. The present study evaluates the effects of a controlled ICP variation on CrCP and RAP among patients with ABI.
Methods: Consecutive neurocritical patients with ICP monitoring were included along with transcranial Doppler and invasive arterial blood pressure monitoring. Internal jugular veins compression was performed for 60 s for the elevation of intracranial blood volume and ICP. Patients were separated in groups according to previous intracranial hypertension severity, with either no skull opening (Sk1), neurosurgical mass lesions evacuation, or decompressive craniectomy (DC) (patients with DC [Sk3]).
Results: Among 98 included patients, the correlation between change (Δ) in ICP and the corresponding ΔCrCP was strong (group Sk1 r = 0.643 [p = 0.0007], group with neurosurgical mass lesions evacuation r = 0.732 [p < 0.0001], and group Sk3 r = 0.580 [p = 0.003], respectively). Patients from group Sk3 presented a significantly higher ΔRAP (p = 0.005); however, for this group, a higher response in mean arterial pressure (change in mean arterial pressure p = 0.034) was observed. Exclusively, group Sk1 disclosed reduction in ICP before internal jugular veins compression withholding.
Conclusions: This study elucidates that CrCP reliably changes in accordance with ICP, being useful to indicate ideal CPP in neurocritical settings. In the early days after DC, cerebrovascular resistance seems to remain elevated, despite exacerbated arterial blood pressure responses in efforts to maintain CPP stable. Patients with ABI with no need of surgical procedures appear to remain with more effective ICP compensatory mechanisms when compared with those who underwent neurosurgical interventions.
Trial registration: ClinicalTrials.gov NCT03694678.
Keywords: Acute brain injury; Cerebral perfusion pressure; Critical closing pressure; Intracranial compliance; Intracranial pressure; Resistance-area product.
© 2023. The Author(s).
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures



References
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
