

Management of left-sided malignant colorectal obstructions with curative intent: a network meta-analysis
- PMID: 36869265
- PMCID: PMC9984133
- DOI: 10.1007/s00464-023-09929-4
Management of left-sided malignant colorectal obstructions with curative intent: a network meta-analysis
Abstract
Background: Several management options exist for colonic decompression in the setting of malignant large bowel obstruction, including oncologic resection, surgical diversion, and SEMS as a bridge-to-surgery. Consensus has yet to be reached on optimal treatment pathways. The aim of the present study was to perform a network meta-analysis comparing short-term postoperative morbidity and long-term oncologic outcomes between oncologic resection, surgical diversion, and self-expanding metal stents (SEMS) in left-sided malignant colorectal obstruction with curative intent.
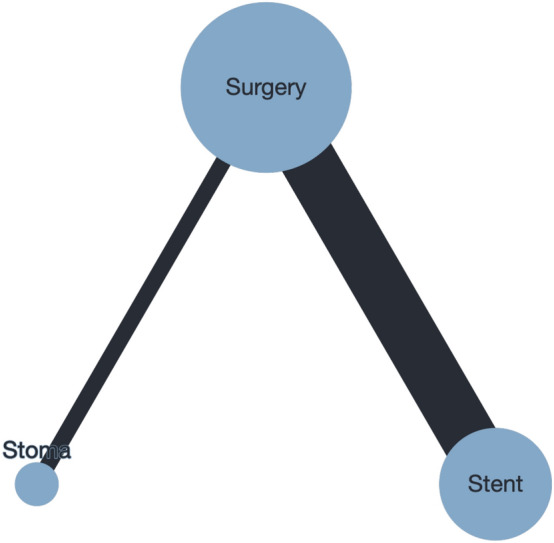
Methods: Medline, Embase, and CENTRAL were systematically searched. Articles were included if they compared two or more of the following in patients presenting with curative left-sided malignant colorectal obstruction: (1) emergent oncologic resection; (2) surgical diversion; and/or (3) SEMS. The primary outcome was overall 90-day postoperative morbidity. Pairwise meta-analyses were performed with inverse variance random effects. Random-effect Bayesian network meta-analysis was performed.
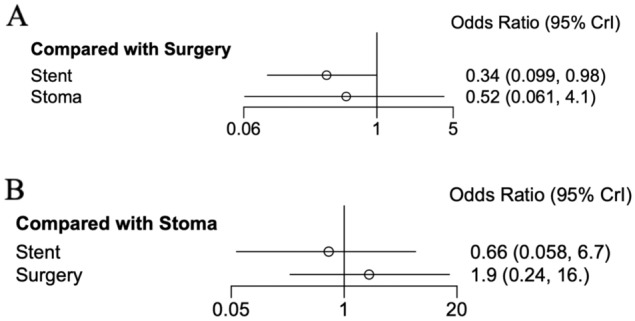
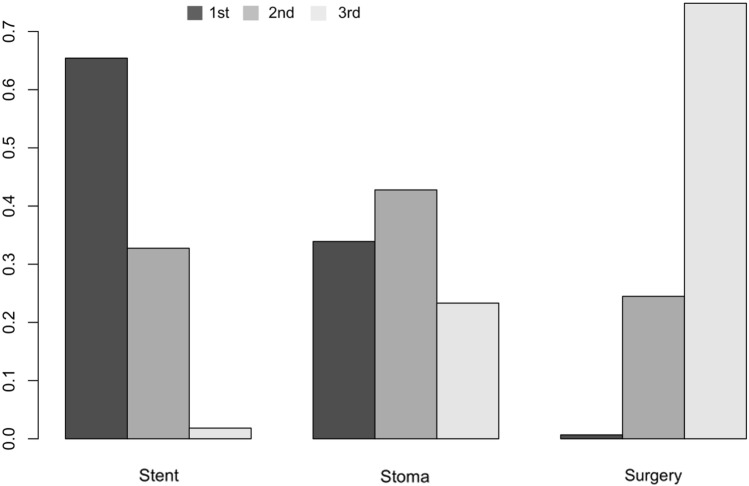
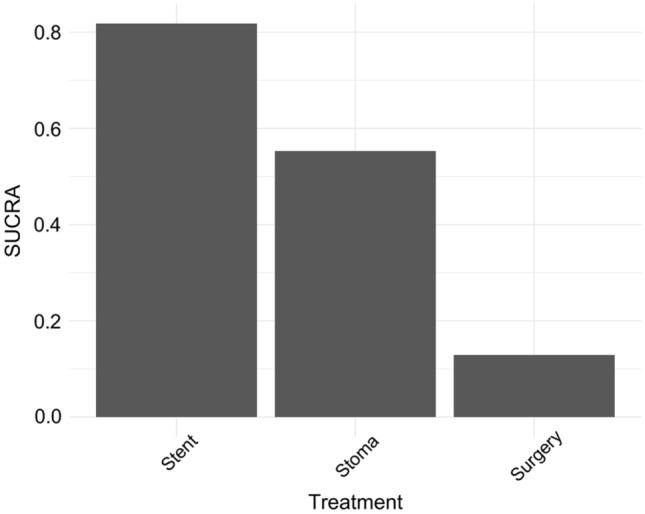
Results: From 1277 citations, 53 studies with 9493 patients undergoing urgent oncologic resection, 1273 patients undergoing surgical diversion, and 2548 patients undergoing SEMS were included. Network meta-analysis demonstrated a significant improvement in 90-day postoperative morbidity in patients undergoing SEMS compared to urgent oncologic resection (OR0.34, 95%CrI0.01-0.98). Insufficient RCT data pertaining to overall survival (OS) precluded network meta-analysis. Pairwise meta-analysis demonstrated decreased five-year OS for patients undergoing urgent oncologic resection compared to surgical diversion (OR0.44, 95%CI0.28-0.71, p < 0.01).
Conclusions: Bridge-to-surgery interventions may offer short- and long-term benefits compared to urgent oncologic resection for malignant colorectal obstruction and should be increasingly considered in this patient population. Further prospective study comparing surgical diversion and SEMS is needed.
Keywords: Colectomy; Colonic Stenting; Colorectal Cancer; Loop Colostomy; Malignant Colorectal Obstruction.
© 2023. The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature.
Conflict of interest statement
Drs. Tyler McKechnie, Jeremy Springer, Zacharie Cloutier, Victoria Archer, Karim Alavi, Aristithes Doumouras, Dennis Hong, and Cagla Eskicioglu have no conflicts of interest or financial ties to disclose.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
