

Non-Invasive Vagus Nerve Stimulation Improves Brain Lesion Volume and Neurobehavioral Outcomes in a Rat Model of Traumatic Brain Injury
- PMID: 36869619
- PMCID: PMC10294566
- DOI: 10.1089/neu.2022.0153
Non-Invasive Vagus Nerve Stimulation Improves Brain Lesion Volume and Neurobehavioral Outcomes in a Rat Model of Traumatic Brain Injury
Abstract
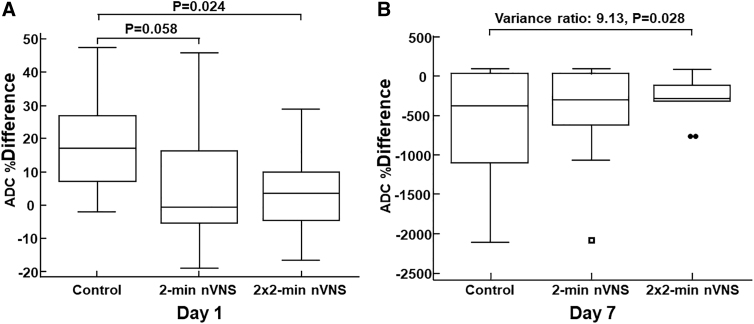
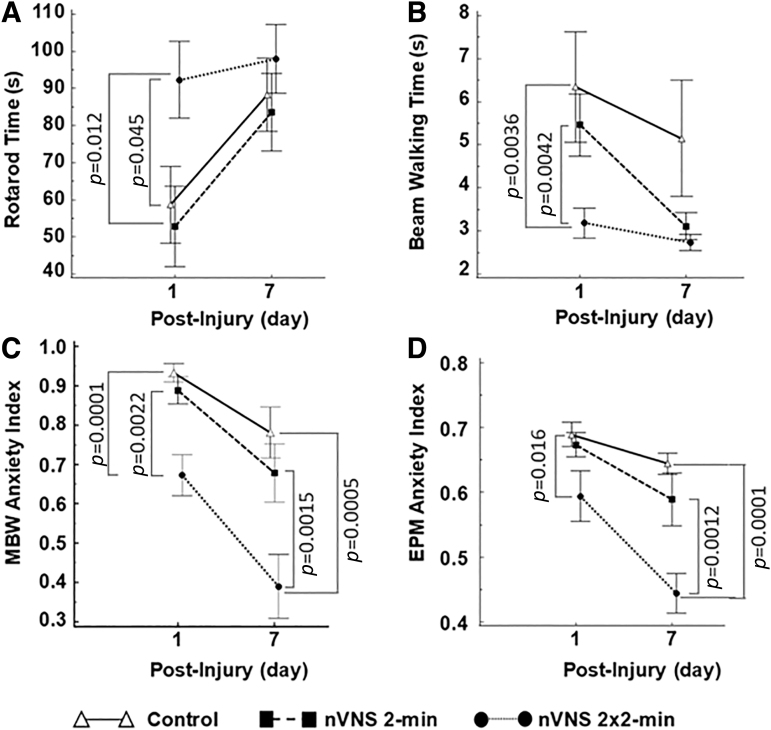
Abstract Traumatic brain injury (TBI) continues to be a major cause of death and disability worldwide. This study assessed the effectiveness of non-invasive vagus nerve stimulation (nVNS) in reducing brain lesion volume and improving neurobehavioral performance in a rat model of TBI. Animals were randomized into three experimental groups: (1) TBI with sham stimulation treatment (Control), (2) TBI treated with five lower doses (2-min) nVNS, and (3) TBI treated with five higher doses (2 × 2-min) nVNS. We used the gammaCore nVNS device to deliver stimulations. Magnetic resonance imaging studies were performed 1 and 7 days post-injury to confirm lesion volume. We observed smaller brain lesion volume in the lower dose nVNS group compared with the control group on days 1 and 7. The lesion volume for the higher dose nVNS group was significantly smaller than either the lower dose nVNS or the control groups on days 1 and 7 post-injury. The apparent diffusion coefficient differences between the ipsilateral and contralateral hemispheres on day 1 were significantly smaller for the higher dose (2 × 2 min) nVNS group than for the control group. Voxel-based morphometry analysis revealed an increase in the ipsilateral cortical volume in the control group caused by tissue deformation and swelling. On day 1, these abnormal volume changes were 13% and 55% smaller in the lower dose and higher dose nVNS groups, respectively, compared with the control group. By day 7, nVNS dampened cortical volume loss by 35% and 89% in the lower dose and higher dose nVNS groups, respectively, compared with the control group. Rotarod, beam walking, and anxiety performances were significantly improved in the higher-dose nVNS group on day 1 compared with the control group. The anxiety indices were also improved on day 7 post-injury compared with the control and the lower-dose nVNS groups. In conclusion, the higher dose nVNS (five 2 × 2-min stimulations) reduced brain lesion volume to a level that further refined the role of nVNS therapy for the acute treatment of TBI. Should nVNS prove effective in additional pre-clinical TBI models and later in clinical settings, it would have an enormous impact on the clinical practice of TBI in both civilian and military settings, as it can easily be adopted into routine clinical practice.
Keywords: brain lesion volume; magnetic resonance imaging; neurobehavioral outcomes; neuromodulation; traumatic brain injury; vagus nerve stimulation.
Conflict of interest statement
Eric Liebler is an employee of electroCore, Inc. Pascal Salazar is an employee of Canon Medical Informatics, Inc. The other authors have nothing to disclose.
Figures




References
-
- Centers for Disease Control and Prevention. Report to Congress on Traumatic Brain Injury in the United States: Epidemiology and Rehabilitation. Atlanta: National Center for Injury Prevention and Control, Division of Unintentional Injury Prevention; 2014.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
