

Yield and Efficiency of a Population-Based Mass Tuberculosis Screening Intervention Among Persons With Diabetes in Jiangsu Province, China
- PMID: 36869807
- PMCID: PMC10320136
- DOI: 10.1093/cid/ciad118
Yield and Efficiency of a Population-Based Mass Tuberculosis Screening Intervention Among Persons With Diabetes in Jiangsu Province, China
Abstract
Background: The evidence-base for mass tuberculosis screening among persons with diabetes (PWD) is poor. We evaluated the yield and costs of mass screening among PWD in eastern China.
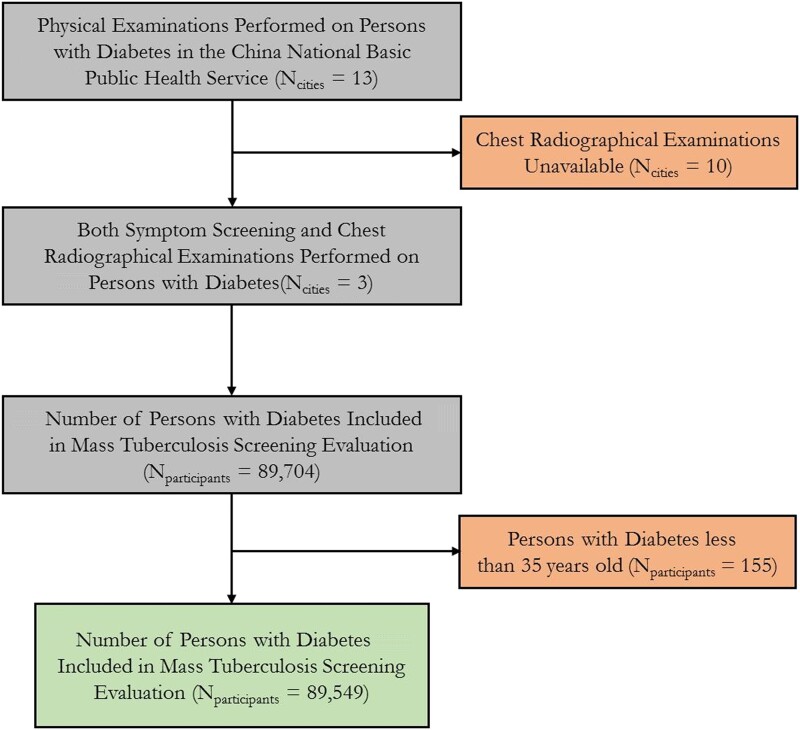
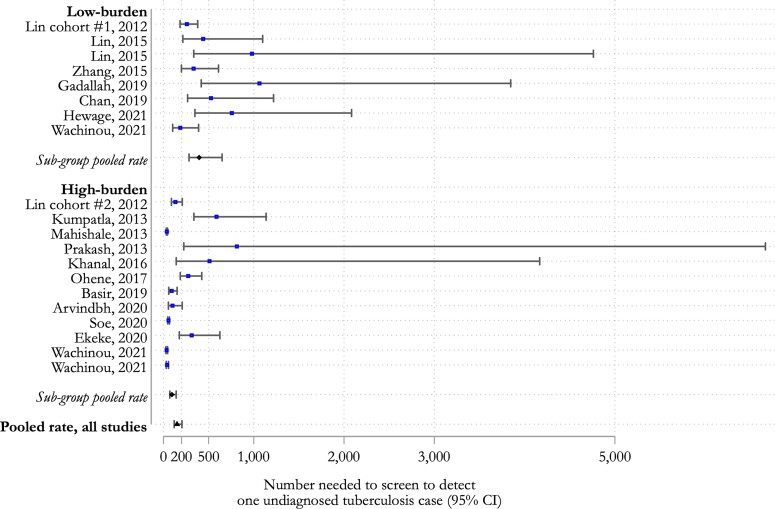
Methods: We included individuals with type 2 diabetes from 38 townships in Jiangsu Province. Screening comprised of physical examinations, symptom screening, and chest X-rays; smear and culture testing were performed through clinical triage. We assessed the yield and number needed to screen (NNS) to detect 1 tuberculosis case among all PWD, those with symptoms, and with suggestive chest X-rays. Unit costing was collected to estimate screening costs and to calculate cost per case detected. We performed a systematic review of other mass tuberculosis screening programs concentrated on PWD.
Results: Of 89 549 screened PWD, 160 were diagnosed with tuberculosis (179 cases per 100 000 persons; 95% confidence interval [CI]: 153-205). The NNS was 560 (95% CI: 513-606), 248 (95% CI: 217-279), and 36 (95% CI: 24-48) among all participants, with abnormal chest X-rays, and symptoms. The cost per case was high overall (US$13 930) but lower with symptoms (US$1037) and high fasting blood glucose levels (US$6807). From systematic review, the pooled NNS to detect one case among all PWD (regardless of symptoms or chest X-ray results) in high- versus low-burden settings was 93 (95% CI: 70-141) versus 395 (95% CI: 283-649).
Conclusions: A mass tuberculosis screening program focused on PWD was feasible however, the overall yield was low and not cost-efficient. Risk-stratified approaches may be practical among PWD in low- and medium tuberculosis burden settings.
Keywords: cost efficiency; diabetes; screening; tuberculosis; yield.
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. The authors: No reported conflicts of interest. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures

Similar articles
-
Mass Tuberculosis Screening Among the Elderly: A Population-Based Study in a Well-Confined, Rural County in Eastern China.Clin Infect Dis. 2023 Nov 17;77(10):1468-1475. doi: 10.1093/cid/ciad438. Clin Infect Dis. 2023. PMID: 37506258 Free PMC article.
-
Comparison of yield and relative costs of different screening algorithms for tuberculosis in active case-finding: a cross-section study.BMC Infect Dis. 2021 Aug 13;21(1):813. doi: 10.1186/s12879-021-06486-w. BMC Infect Dis. 2021. PMID: 34388976 Free PMC article.
-
Comparing yield and relative costs of WHO TB screening algorithms in selected risk groups among people aged 65 years and over in China, 2013.PLoS One. 2017 Jun 8;12(6):e0176581. doi: 10.1371/journal.pone.0176581. eCollection 2017. PLoS One. 2017. PMID: 28594824 Free PMC article.
-
Screening tests for active pulmonary tuberculosis in children.Cochrane Database Syst Rev. 2021 Jun 28;6(6):CD013693. doi: 10.1002/14651858.CD013693.pub2. Cochrane Database Syst Rev. 2021. PMID: 34180536 Free PMC article.
-
Number Needed to Screen for Tuberculosis Disease Among Children: A Systematic Review.Pediatrics. 2023 Apr 1;151(4):e2022059189. doi: 10.1542/peds.2022-059189. Pediatrics. 2023. PMID: 36987808 Free PMC article.
Cited by
-
Prospective cohort study on tuberculosis incidence and risk factors in the elderly population of eastern China.Heliyon. 2024 Jan 19;10(3):e24507. doi: 10.1016/j.heliyon.2024.e24507. eCollection 2024 Feb 15. Heliyon. 2024. PMID: 38314308 Free PMC article.
-
Development of chronic obstructive pulmonary disease after a tuberculosis episode in a large, population-based cohort from Eastern China.Int J Epidemiol. 2025 Feb 16;54(2):dyae174. doi: 10.1093/ije/dyae174. Int J Epidemiol. 2025. PMID: 39993264
-
Mass Tuberculosis Screening Among the Elderly: A Population-Based Study in a Well-Confined, Rural County in Eastern China.Clin Infect Dis. 2023 Nov 17;77(10):1468-1475. doi: 10.1093/cid/ciad438. Clin Infect Dis. 2023. PMID: 37506258 Free PMC article.
-
Spatial-temporal distribution characteristics of pulmonary tuberculosis in eastern China from 2011 to 2021.Epidemiol Infect. 2024 May 15;152:e84. doi: 10.1017/S0950268824000785. Epidemiol Infect. 2024. PMID: 38745412 Free PMC article.
References
-
- Beagley J, Guariguata L, Weil C, Motala AA. Global estimates of undiagnosed diabetes in adults. Diabetes Res Clin Pract 2014; 103:150–60. - PubMed
-
- Odone A, Houben RM, White RG, Lönnroth K. The effect of diabetes and undernutrition trends on reaching 2035 global tuberculosis targets. Lancet Diabetes Endocrinol 2014; 2:754–64. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
