

The prevalence, correlation, and co-occurrence of neuropathology in old age: harmonisation of 12 measures across six community-based autopsy studies of dementia
- PMID: 36870337
- PMCID: PMC9977689
- DOI: 10.1016/S2666-7568(23)00019-3
The prevalence, correlation, and co-occurrence of neuropathology in old age: harmonisation of 12 measures across six community-based autopsy studies of dementia
Abstract
Background: Population-based autopsy studies provide valuable insights into the causes of dementia but are limited by sample size and restriction to specific populations. Harmonisation across studies increases statistical power and allows meaningful comparisons between studies. We aimed to harmonise neuropathology measures across studies and assess the prevalence, correlation, and co-occurrence of neuropathologies in the ageing population.
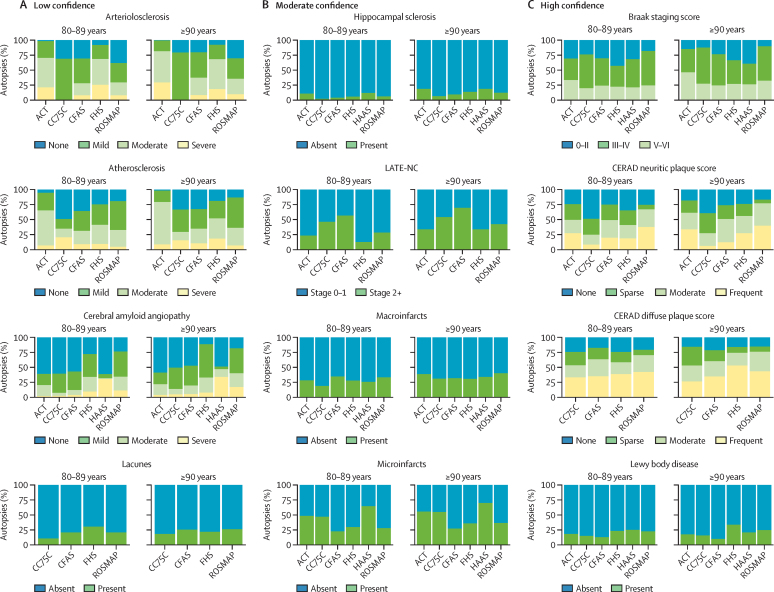
Methods: We combined data from six community-based autopsy cohorts in the US and the UK in a coordinated cross-sectional analysis. Among all decedents aged 80 years or older, we assessed 12 neuropathologies known to be associated with dementia: arteriolosclerosis, atherosclerosis, macroinfarcts, microinfarcts, lacunes, cerebral amyloid angiopathy, Braak neurofibrillary tangle stage, Consortium to Establish a Registry for Alzheimer's disease (CERAD) diffuse plaque score, CERAD neuritic plaque score, hippocampal sclerosis, limbic-predominant age-related TDP-43 encephalopathy neuropathologic change (LATE-NC), and Lewy body pathology. We divided measures into three groups describing level of confidence (low, moderate, and high) in harmonisation. We described the prevalence, correlations, and co-occurrence of neuropathologies.
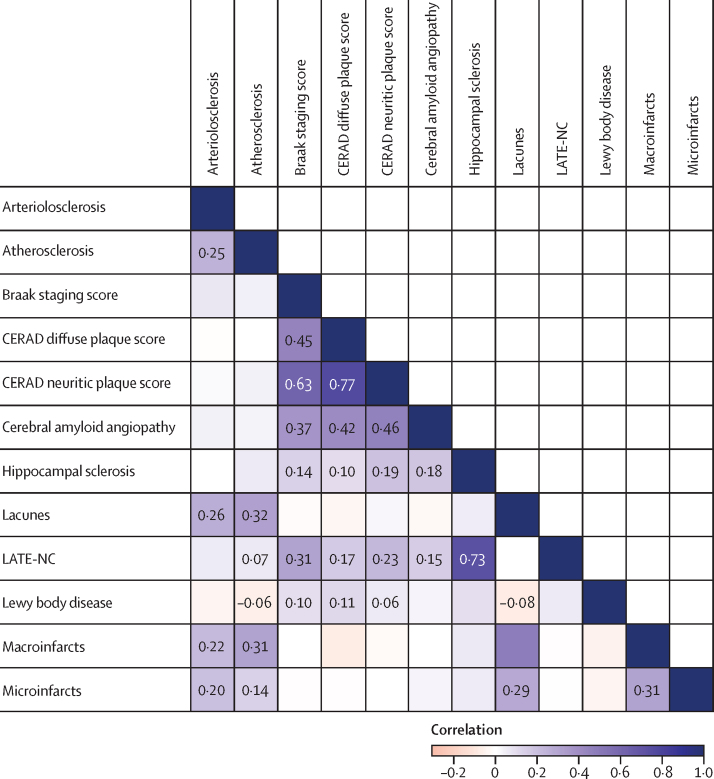
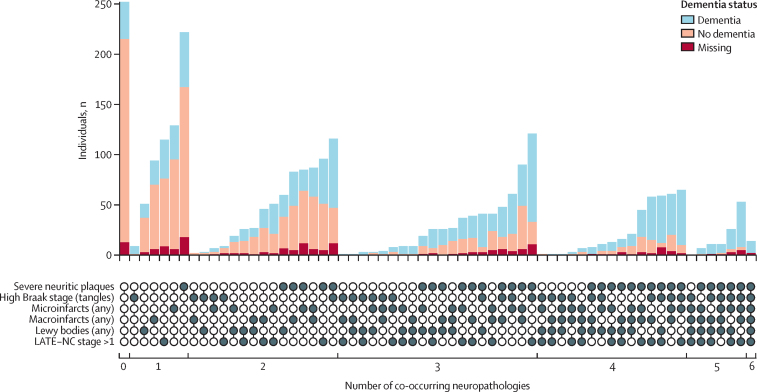
Findings: The cohorts included 4354 decedents aged 80 years or older with autopsy data. All cohorts included more women than men, with the exception of one study that only included men, and all cohorts included decedents at older ages (range of mean age at death across cohorts 88·0-91·6 years). Measures of Alzheimer's disease neuropathological change, Braak stage and CERAD scores, were in the high confidence category, whereas measures of vascular neuropathologies were in the low (arterioloscerosis, atherosclerosis, cerebral amyloid angiopathy, and lacunes) or moderate (macroinfarcts and microinfarcts) categories. Neuropathology prevalence and co-occurrence was high (2443 [91%] of 2695 participants had more than one of six key neuropathologies and 1106 [41%] of 2695 had three or more). Co-occurrence was strongly but not deterministically associated with dementia status. Vascular and Alzheimer's disease features clustered separately in correlation analyses, and LATE-NC had moderate associations with Alzheimer's disease measures (eg, Braak stage ρ=0·31 [95% CI 0·20-0·42]).
Interpretation: Higher variability and more inconsistency in the measurement of vascular neuropathologies compared with the measurement of Alzheimer's disease neuropathological change suggests the development of new frameworks for the measurement of vascular neuropathologies might be helpful. Results highlight the complexity and multi-morbidity of the brain pathologies that underlie dementia in older adults and suggest that prevention efforts and treatments should be multifaceted.
Funding: Gates Ventures.
Copyright © 2023 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests SS reports consulting fees from Biogen and Eisai. JS reports consulting fees from AVID, Alnylam Pharmaceuticals, and Cerveau Technologies. All other authors declare no competing interests.
Figures
Comment in
-
Autopsy studies are key to identifying dementia cause.Lancet Healthy Longev. 2023 Mar;4(3):e94-e95. doi: 10.1016/S2666-7568(23)00022-3. Lancet Healthy Longev. 2023. PMID: 36870340 No abstract available.
References
-
- Ferrari C, Sorbi S. The complexity of Alzheimer's disease: an evolving puzzle. Physiol Rev. 2021;101:1047–1081. - PubMed
-
- Mullane K, Williams M. Alzheimer's disease beyond amyloid: Can the repetitive failures of amyloid-targeted therapeutics inform future approaches to dementia drug discovery? Biochem Pharmacol. 2020;177 - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
- UH3 NS100599/NS/NINDS NIH HHS/United States
- R01 AG054076/AG/NIA NIH HHS/United States
- RF1 AG059421/AG/NIA NIH HHS/United States
- HHSN268201500001C/HL/NHLBI NIH HHS/United States
- R01 AG062531/AG/NIA NIH HHS/United States
- R01 AG049607/AG/NIA NIH HHS/United States
- U01 AG019349/AG/NIA NIH HHS/United States
- G0601022/MRC_/Medical Research Council/United Kingdom
- R01 AG066524/AG/NIA NIH HHS/United States
- HHSN268201500001I/HL/NHLBI NIH HHS/United States
- P30 AG066509/AG/NIA NIH HHS/United States
- U01 AG006781/AG/NIA NIH HHS/United States
- K08 AG065426/AG/NIA NIH HHS/United States
- 75N92019D00031/HL/NHLBI NIH HHS/United States
- U19 AG066567/AG/NIA NIH HHS/United States
- R01 AG015819/AG/NIA NIH HHS/United States
- G0900582/MRC_/Medical Research Council/United Kingdom
- R01 NS017950/NS/NINDS NIH HHS/United States
- UF1 NS125513/NS/NINDS NIH HHS/United States
- N01 HC005102/HC/NHLBI NIH HHS/United States
- DH_/Department of Health/United Kingdom
- U.1052.00.0013/MRC_/Medical Research Council/United Kingdom
- R01 NS041265/NS/NINDS NIH HHS/United States
- R01 AG017917/AG/NIA NIH HHS/United States
- G9901400/MRC_/Medical Research Council/United Kingdom
- P30 AG010161/AG/NIA NIH HHS/United States
- N01 HC025195/HL/NHLBI NIH HHS/United States
- P30 AG066546/AG/NIA NIH HHS/United States
- P30 AG044271/AG/NIA NIH HHS/United States
- G0400077/MRC_/Medical Research Council/United Kingdom
- R01 AG017155/AG/NIA NIH HHS/United States
