

CDK4/6 inhibition triggers ICAM1-driven immune response and sensitizes LKB1 mutant lung cancer to immunotherapy
- PMID: 36871040
- PMCID: PMC9985635
- DOI: 10.1038/s41467-023-36892-4
CDK4/6 inhibition triggers ICAM1-driven immune response and sensitizes LKB1 mutant lung cancer to immunotherapy
Abstract
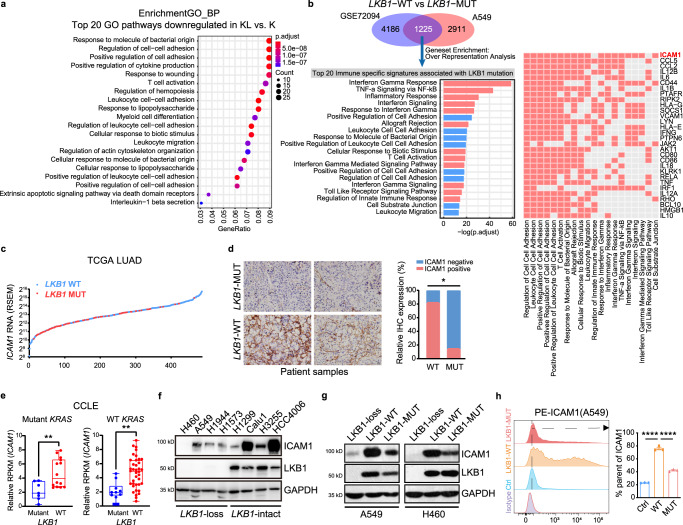
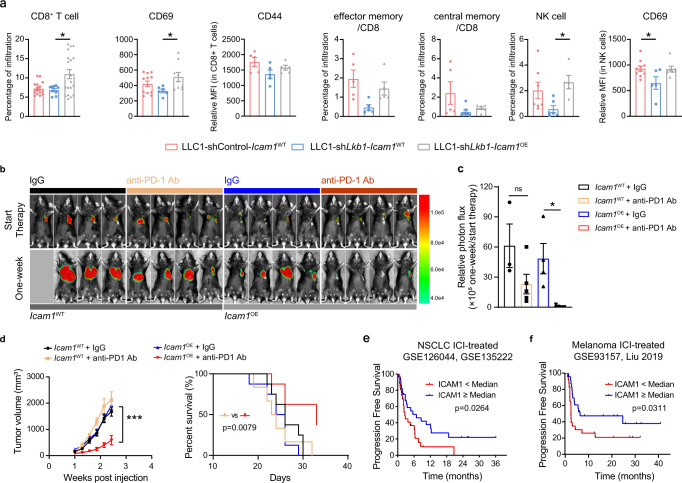
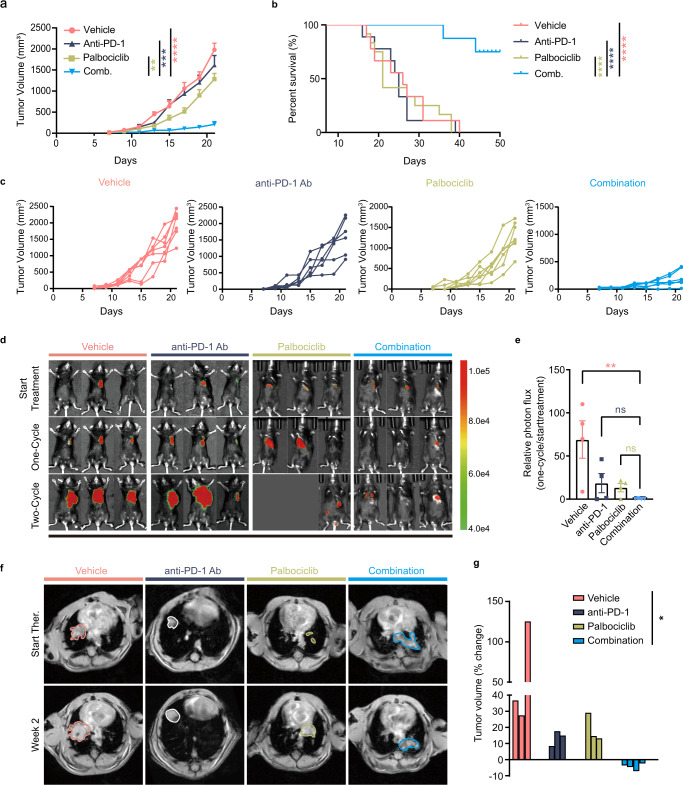
Liver kinase B1 (LKB1) mutation is prevalent and a driver of resistance to immune checkpoint blockade (ICB) therapy for lung adenocarcinoma. Here leveraging single cell RNA sequencing data, we demonstrate that trafficking and adhesion process of activated T cells are defected in genetically engineered Kras-driven mouse model with Lkb1 conditional knockout. LKB1 mutant cancer cells result in marked suppression of intercellular adhesion molecule-1 (ICAM1). Ectopic expression of Icam1 in Lkb1-deficient tumor increases homing and activation of adoptively transferred SIINFEKL-specific CD8+ T cells, reactivates tumor-effector cell interactions and re-sensitises tumors to ICB. Further discovery proves that CDK4/6 inhibitors upregulate ICAM1 transcription by inhibiting phosphorylation of retinoblastoma protein RB in LKB1 deficient cancer cells. Finally, a tailored combination strategy using CDK4/6 inhibitors and anti-PD-1 antibodies promotes ICAM1-triggered immune response in multiple Lkb1-deficient murine models. Our findings renovate that ICAM1 on tumor cells orchestrates anti-tumor immune response, especially for adaptive immunity.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures





References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
