

Long-term adherence to healthful and unhealthful plant-based diets and breast cancer risk overall and by hormone receptor and histologic subtypes among postmenopausal females
- PMID: 36872016
- PMCID: PMC10131618
- DOI: 10.1016/j.ajcnut.2022.11.019
Long-term adherence to healthful and unhealthful plant-based diets and breast cancer risk overall and by hormone receptor and histologic subtypes among postmenopausal females
Abstract
Background: Epidemiological studies assessing the influence of vegetarian diets on breast cancer (BC) risk have produced inconsistent results. Few studies have assessed how the incremental decrease in animal foods and the quality of plant foods are linked with BC.
Objectives: Disentangle the influence of plant-based diet quality on BC risk between postmenopausal females.
Methods: Total of 65,574 participants from the E3N (Etude Epidémiologique auprès de femmes de la Mutuelle Générale de l'Education Nationale) cohort were followed from 1993-2014. Incident BC cases were confirmed through pathological reports and classified into subtypes. Cumulative average scores for healthful (hPDI) and unhealthful (uPDI) plant-based diet indices were developed using self-reported dietary intakes at baseline (1993) and follow-up (2005) and divided into quintiles. Cox proportional hazards models were used to estimate adjusted HR and 95% CI.
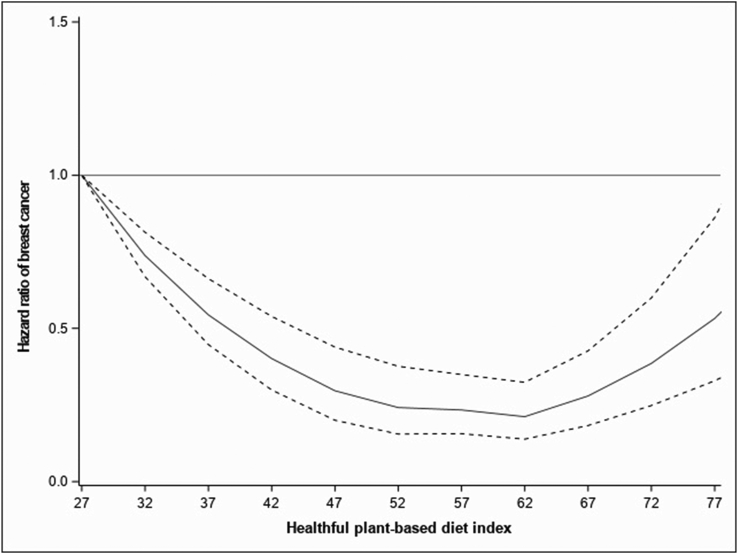
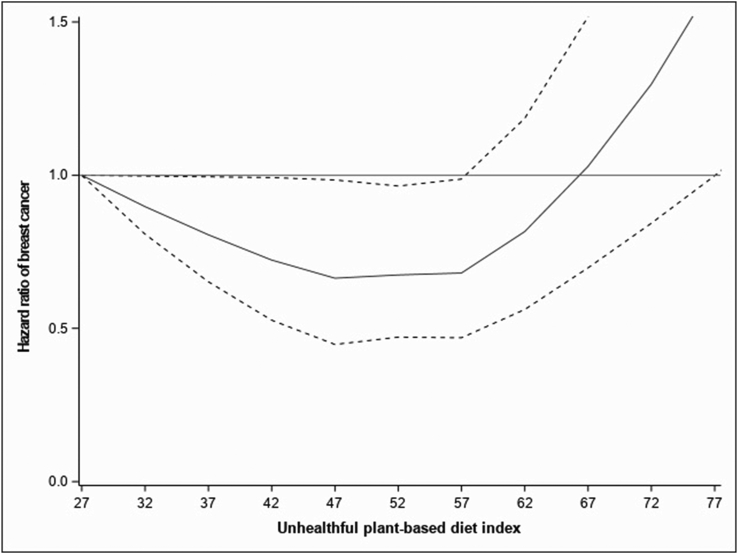
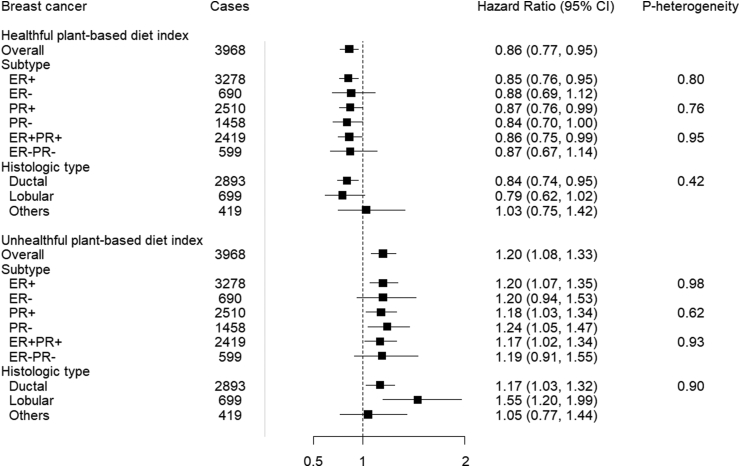
Results: During a mean follow-up of 21 y, 3968 incident postmenopausal BC cases were identified. There was a nonlinear association between adherence to hPDI and BC risk (Pnonlinear < 0.01). Compared to participants with low adherence to hPDI, those with high adherence had a lower BC risk [HRQ3 compared withQ1 (95% CI): 0.79 (0.71, 0.87) and HRQ4 compared with Q1 (95% CI): 0.78 (0.70, 0.86)]. In contrast, higher adherence to unhealthful was associated with a linear increase in BC risk [Pnonlinear = 0.18; HRQ5 compared with Q1 (95% CI): 1.20 (1.08, 1.33); Ptrend < 0.01]. Associations were similar according to BC subtypes (Pheterogeneity > 0.05 for all).
Conclusions: Long-term adherence to healthful plant foods with some intake of unhealthy plant and animal foods may reduce BC risk with an optimal risk reduction in the moderate intake range. Adherence to an unhealthful plant-based diet may increase BC risk. These results emphasize the importance of the quality of plant foods for cancer prevention. This trial was registered at clinicaltrials.gov (NCT03285230).
Keywords: breast cancer; dietary score; estrogen receptor; plant-based diet quality; progesterone receptor; prospective study.
Copyright © 2022. Published by Elsevier Inc.
Figures
Comment in
-
For breast cancer prevention, not all plant-based diets are created equal.Am J Clin Nutr. 2023 Mar;117(3):453-454. doi: 10.1016/j.ajcnut.2022.12.017. Am J Clin Nutr. 2023. PMID: 36872015 No abstract available.
References
-
- Fitzmaurice C., Allen C., Barber R.M., Barregard L., Bhutta Z.A., Brenner H., et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 32 cancer groups, 1990 to 2015: A systematic analysis for the global burden of disease study. JAMA Oncol. 2017;3(4):524–548. doi: 10.1001/jamaoncol.2016.5688. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
