

Immunogenicity of CRISPR therapeutics-Critical considerations for clinical translation
- PMID: 36873375
- PMCID: PMC9978118
- DOI: 10.3389/fbioe.2023.1138596
Immunogenicity of CRISPR therapeutics-Critical considerations for clinical translation
Abstract
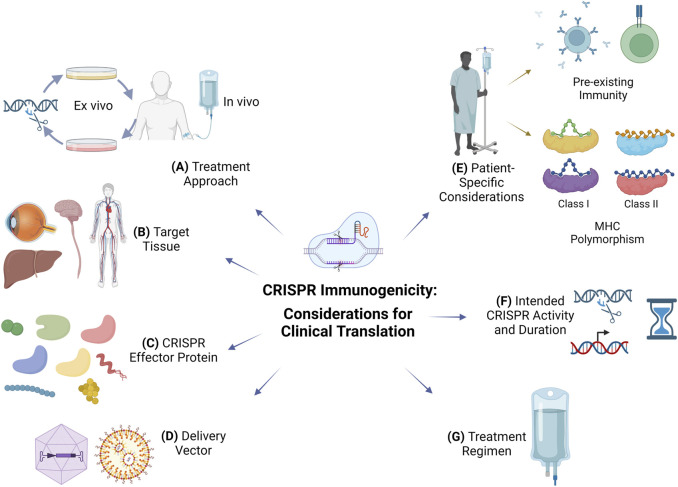
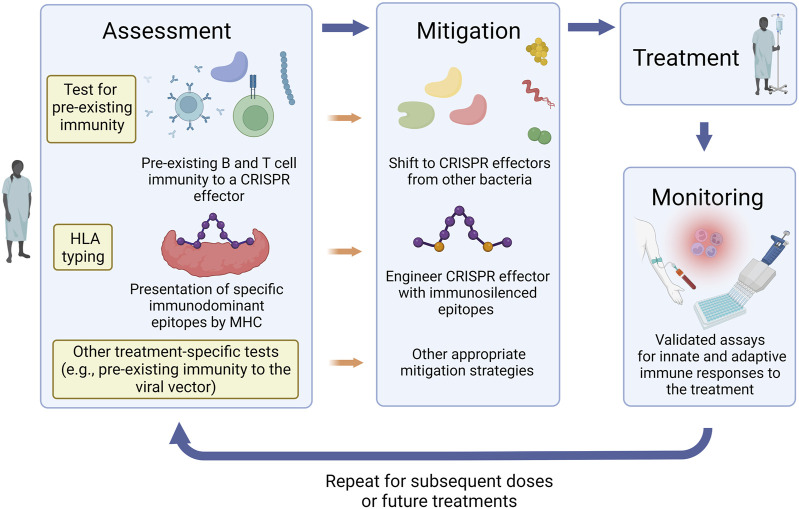
CRISPR offers new hope for many patients and promises to transform the way we think of future therapies. Ensuring safety of CRISPR therapeutics is a top priority for clinical translation and specific recommendations have been recently released by the FDA. Rapid progress in the preclinical and clinical development of CRISPR therapeutics leverages years of experience with gene therapy successes and failures. Adverse events due to immunogenicity have been a major setback that has impacted the field of gene therapy. As several in vivo CRISPR clinical trials make progress, the challenge of immunogenicity remains a significant roadblock to the clinical availability and utility of CRISPR therapeutics. In this review, we examine what is currently known about the immunogenicity of CRISPR therapeutics and discuss several considerations to mitigate immunogenicity for the design of safe and clinically translatable CRISPR therapeutics.
Keywords: CRISPR-Cas; Cas9; clinical translation; clinical trials; gene therapy; genome editing; immunogenicity.
Copyright © 2023 Ewaisha and Anderson.
Conflict of interest statement
RE and KSA are noted as inventors on a patent regarding Cas9 immunity.
Figures
Similar articles
-
Lipid-Nanoparticle-Based Delivery of CRISPR/Cas9 Genome-Editing Components.Mol Pharm. 2022 Jun 6;19(6):1669-1686. doi: 10.1021/acs.molpharmaceut.1c00916. Epub 2022 May 20. Mol Pharm. 2022. PMID: 35594500 Free PMC article. Review.
-
Ex vivo cell-based CRISPR/Cas9 genome editing for therapeutic applications.Biomaterials. 2020 Mar;234:119711. doi: 10.1016/j.biomaterials.2019.119711. Epub 2020 Jan 10. Biomaterials. 2020. PMID: 31945616 Free PMC article. Review.
-
Key considerations in designing CRISPR/Cas9-carrying nanoparticles for therapeutic genome editing.Nanoscale. 2020 Oct 29;12(41):21001-21014. doi: 10.1039/d0nr05452f. Nanoscale. 2020. PMID: 33078813 Review.
-
Delivering the CRISPR/Cas9 system for engineering gene therapies: Recent cargo and delivery approaches for clinical translation.Front Bioeng Biotechnol. 2022 Sep 26;10:973326. doi: 10.3389/fbioe.2022.973326. eCollection 2022. Front Bioeng Biotechnol. 2022. PMID: 36225598 Free PMC article. Review.
-
Pre-clinical non-viral vectors exploited for in vivo CRISPR/Cas9 gene editing: an overview.Biomater Sci. 2022 Jun 28;10(13):3410-3432. doi: 10.1039/d1bm01452h. Biomater Sci. 2022. PMID: 35604372 Review.
Cited by
-
Control of HSV-1 Infection: Directions for the Development of CRISPR/Cas-Based Therapeutics and Diagnostics.Int J Mol Sci. 2024 Nov 17;25(22):12346. doi: 10.3390/ijms252212346. Int J Mol Sci. 2024. PMID: 39596412 Free PMC article. Review.
-
Challenges and Considerations of Preclinical Development for iPSC-Based Myogenic Cell Therapy.Cells. 2024 Mar 29;13(7):596. doi: 10.3390/cells13070596. Cells. 2024. PMID: 38607035 Free PMC article. Review.
-
Targeted DNA Methylation Using Modified DNA Probes: A Potential Therapeutic Tool for Depression and Stress-Related Disorders.Int J Mol Sci. 2025 Jun 12;26(12):5643. doi: 10.3390/ijms26125643. Int J Mol Sci. 2025. PMID: 40565107 Free PMC article.
-
Progress and pitfalls of gene editing technology in CAR-T cell therapy: a state-of-the-art review.Front Oncol. 2024 Jun 7;14:1388475. doi: 10.3389/fonc.2024.1388475. eCollection 2024. Front Oncol. 2024. PMID: 38912057 Free PMC article. Review.
-
Enhancing precision in cancer treatment: the role of gene therapy and immune modulation in oncology.Front Med (Lausanne). 2025 Jan 13;11:1527600. doi: 10.3389/fmed.2024.1527600. eCollection 2024. Front Med (Lausanne). 2025. PMID: 39871848 Free PMC article. Review.
References
-
- Annoni A., Brown B. D., Cantore A., Sergi L. S., Naldini L., Roncarolo M.-G. (2009). In vivo delivery of a microRNA-regulated transgene induces antigen-specific regulatory T cells and promotes immunologic tolerance. Blood, J. Am. Soc. Hematol. 114, 5152–5161. 10.1182/blood-2009-04-214569 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials