

Assessment of the Endotracheal Tube Tip Position by Bedside Ultrasound in a Pediatric Intensive Care Unit: A Cross-sectional Study
- PMID: 36873587
- PMCID: PMC9983650
- DOI: 10.5005/jp-journals-10071-24355
Assessment of the Endotracheal Tube Tip Position by Bedside Ultrasound in a Pediatric Intensive Care Unit: A Cross-sectional Study
Abstract
Introduction: The chest X-ray (CXR) is the standard of practice to assess the tip of the endotracheal tube (ETT) in ventilated children. In many hospitals, it takes hours to get a bedside CXR, and it has radiation exposure. The objective of this study was to find the utility of bedside ultrasound (USG), in assessing the ETT tip position in a Pediatric Intensive Care Unit (PICU).
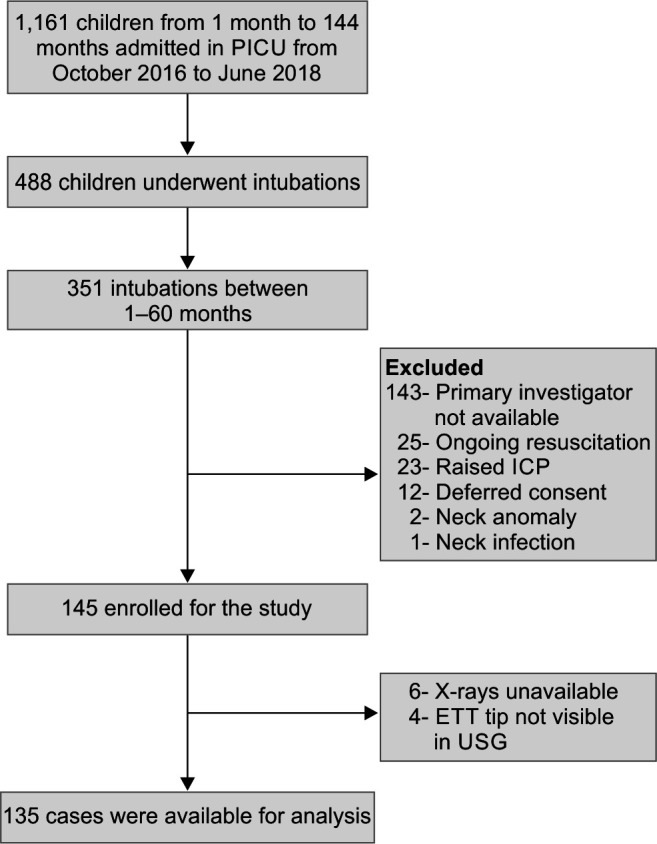
Methods: It was a prospective study conducted in the PICU of a tertiary care center involving 135 children aged from 1 month to 60 months, requiring endotracheal intubation. In this study, the authors compared the position of the ETT tip by the CXR (gold standard) and USG. The CXR was taken in children to assess the correct position of the tip of ETT. The USG was used to measure the distance between the tip of ETT and the arch of the aorta, thrice in the same patient. The mean of the three USG readings was compared with the distance between the tip of the ETT and carina in CXR.
Results: The reliability of three USG readings was tested by absolute agreement coefficient in intraclass correlation (ICC), 0.986 (95% CI: 0.981-0.989). The sensitivity and specificity of the USG in identifying the correct position of the ETT tip in children when compared to CXR were 98.10% (95% CI: 93.297-99.71%) and 50.0% (95% CI: 31.30-68.70%), respectively.
Conclusion: In ventilated children <60 months of age, identifying the tip of ETTs by bedside the USG has good sensitivity (98.10%) but poor specificity (50.0%).
How to cite this article: Subramani S, Parameswaran N, Ananthkrishnan R, Abraham S, Chidambaram M, Rameshkumar R, et al. Assessment of the Endotracheal Tube Tip Position by Bedside Ultrasound in a Pediatric Intensive Care Unit: A Cross-sectional Study. Indian J Crit Care Med 2022;26(11):1218-1224.
Keywords: Bedside ultrasound; Children; Endotracheal tube tip position.
Copyright © 2022; Jaypee Brothers Medical Publishers (P) Ltd.
Conflict of interest statement
Source of support: Nil Conflict of interest: None
Figures



References
Publication types
LinkOut - more resources
Full Text Sources