

Lichen sclerosus: The 2023 update
- PMID: 36873861
- PMCID: PMC9978401
- DOI: 10.3389/fmed.2023.1106318
Lichen sclerosus: The 2023 update
Abstract
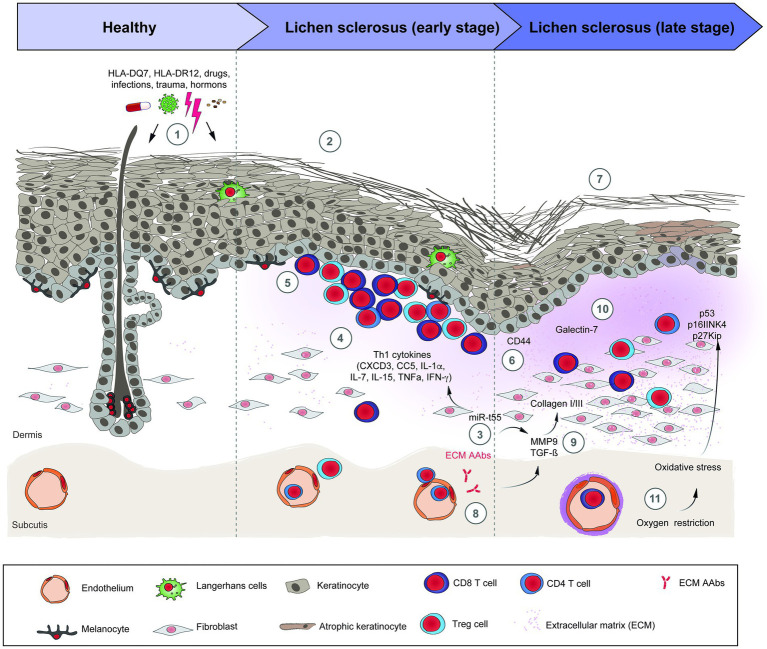
Lichen sclerosus (LS) is an underdiagnosed inflammatory mucocutaneous condition affecting the anogenital areas. Postmenopausal women are predominantly affected and, to a lesser extent, men, prepubertal children, and adolescents. The etiology of LS is still unknown. Hormonal status, frequent trauma and autoimmune diseases are well-known associations for LS, yet infections do not seem to be clear risk factors. LS pathogenesis involves factors such as a genetic predisposition and an immune-mediated Th1-specific IFNγ-induced phenotype. Furthermore, there is a distinct expression of tissue remodeling associated genes as well as microRNAs. Oxidative stress with lipid and DNA peroxidation provides an enabling microenvironment to autoimmunity and carcinogenesis. Circulating IgG autoantibodies against the extracellular matrix protein 1 and hemidesmosome may contribute to the progression of LS or simply represent an epiphenomenon. The typical clinical picture includes chronic whitish atrophic patches along with itching and soreness in the vulvar, perianal and penile regions. In addition to genital scarring, and sexual and urinary dysfunction, LS may also lead to squamous cell carcinoma. Disseminated extragenital LS and oral LS are also reported. The diagnosis is usually clinical; however, a skin biopsy should be performed in case of an unclear clinical picture, treatment failure or suspicion of a neoplasm. The gold-standard therapy is the long-term application of ultrapotent or potent topical corticosteroids and, alternatively, topical calcineurin inhibitors such as pimecrolimus or tacrolimus. Collectively, LS is a common dermatological disease with a so far incompletely understood pathogenesis and only limited treatment options. To foster translational research in LS, we provide here an update on its clinical features, pathogenesis, diagnosis and (emerging) treatment options.
Keywords: autoimmunity; balanitis xerotica obliterans; kraurosis vulvae; lichen sclerosus; white spot disease.
Copyright © 2023 De Luca, Papara, Vorobyev, Staiger, Bieber, Thaçi and Ludwig.
Conflict of interest statement
DT: Honoraria for participation on advisory boards, as a speaker and for consultancy from AbbVie, Almirall, Boehringer Ingelheim, Bristol Myers Squibb, Eli Lilly, Galapagos, Janssen, LEO Pharma, Morphosis, Novartis, Pfizer, Regeneron, Samsung, Sandoz, Sanofi Genzyme, and UCB Pharma; research grants received from LEO Pharma, and Novartis. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Hallopeau H. Leçons cliniques sur les maladies cutanées et syphilitiques. Union Med Can. (1887) 43:472.
-
- Papini M, Russo A, Simonetti O, Borghi A, Corazza M, Piaserico S, et al. . Mucous membrane disorders research group of SIDeMaST. Diagnosis and management of cutaneous and anogenital lichen sclerosus: recommendations from the Italian Society of Dermatology (SIDeMaST). Ital J Dermatol Venerol. (2021) 156:519–33. doi: 10.23736/S2784-8671.21.06764-X, PMID: - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials