

Autoantibodies against citrullinated and native proteins and prediction of rheumatoid arthritis-associated interstitial lung disease: A nested case-control study
- PMID: 36874209
- PMCID: PMC9979957
- DOI: 10.1016/s2665-9913(22)00380-0
Autoantibodies against citrullinated and native proteins and prediction of rheumatoid arthritis-associated interstitial lung disease: A nested case-control study
Abstract
Background: To identify fine specificity anti-citrullinated protein antibodies (ACPA) associated with incident rheumatoid arthritis-associated interstitial lung disease (RA-ILD).
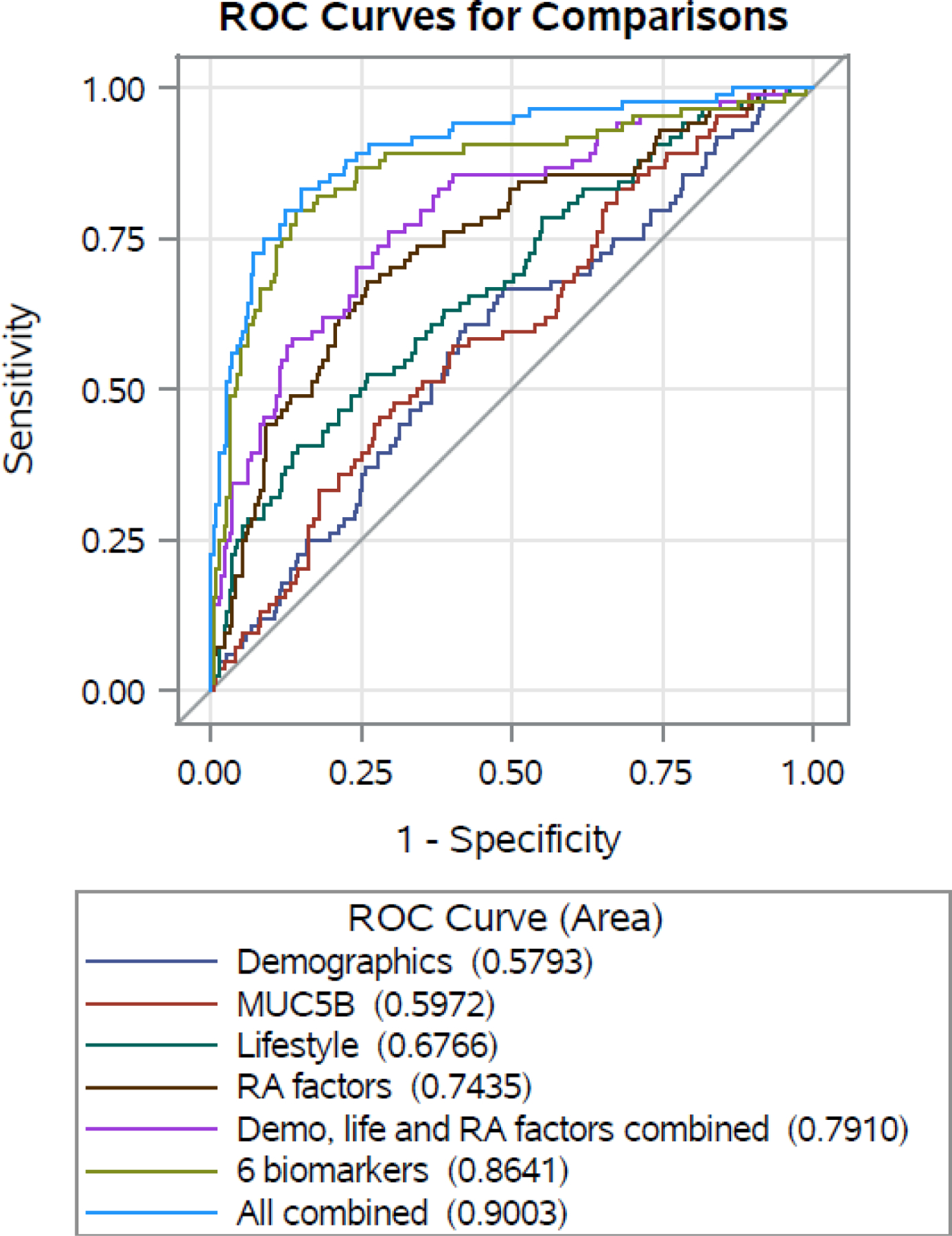
Methods: This nested case-control study within the Brigham RA Sequential Study matched incident RA-ILD cases to RA-noILD controls on time of blood collection, age, sex, RA duration, and rheumatoid factor status. A multiplex assay measured ACPA and anti-native protein antibodies from stored serum prior to RA-ILD onset. Logistic regression models calculated odds ratios (OR) with 95% confidence intervals (CI) for RA-ILD, adjusting for prospectively-collected covariates. We estimated optimism-corrected area under the curves (AUC) using internal validation. Model coefficients generated a risk score for RA-ILD.
Findings: We analyzed 84 incident RA-ILD cases (mean age 67 years, 77% female, 90% White) and 233 RA-noILD controls (mean age 66 years, 80% female, 94% White). We identified six fine specificity antibodies that were associated with RA-ILD. The antibody isotypes and targeted proteins were: IgA2 to citrullinated histone 4 (OR 0.08 per log-transformed unit, 95% CI 0.03-0.22), IgA2 to citrullinated histone 2A (OR 4.03, 95% CI 2.03-8.00), IgG to cyclic citrullinated filaggrin (OR 3.47, 95% CI 1.71-7.01), IgA2 to native cyclic histone 2A (OR 5.52, 95% CI 2.38-12.78), IgA2 to native histone 2A (OR 4.60, 95% CI 2.18-9.74), and IgG to native cyclic filaggrin (OR 2.53, 95% CI 1.47-4.34). These six antibodies predicted RA-ILD risk better than all clinical factors combined (optimism-corrected AUC=0·84 versus 0·73). We developed a risk score for RA-ILD combining these antibodies with the clinical factors (smoking, disease activity, glucocorticoid use, obesity). At 50% predicted RA-ILD probability, the risk scores both without (score=2·6) and with (score=5·9) biomarkers achieved specificity ≥93% for RA-ILD.
Interpretation: Specific ACPA and anti-native protein antibodies improve RA-ILD prediction. These findings implicate synovial protein antibodies in the pathogenesis of RA-ILD and suggest clinical utility in predicting RA-ILD once validated in external studies.
Funding: National Institutes of Health.
Conflict of interest statement
Declaration of interests: Dr. Yoshida has received consulting fees from OM1 unrelated to this work. Dr. Davis has received research support from Pfizer, has a patent pending for assessing and treating arthritis and serve on a data safety monitoring board for a rheumatoid arthritis clinical trial sponsored by the National Institutes of Health, all unrelated to this work. Dr. Dellaripa has received consulting fees from Boehringer Ingelheim, Bristol Myers Squibb, and Genentech and receives royalties from UpToDate unrelated to this work. Dr. Hatabu has received research support from Canon Medical Systems and Konica-Minolta as well as consulting fees from Canon Medical Systems and the Mitsubishi Chemical Company unrelated to this work. Dr. Nishino has received research support from AstraZeneca, Canon Medical Systems, and Daiichi Sankyo, and consulting fees from AstraZeneca, Daiichi Sankyo unrelated to this work. Dr. Sokolove is currently an employee at GlaxoSmithKline and owns shares in GlaxoSmithKline, and his work on this project preceded this employment. Dr. Weinblatt has received research support from Amgen, Bristol Myers Squibb, Eli Lilly, Aqtual, and Janssen; consultancy fees from AbbVie, Aclaris, Amgen, Aqtual, Bayer, Bristol Myers Squibb, CorEvitas, EqRX, Genosco, GlaxoSmithKline, Gilead, Johnson & Johnson, Kyvrena, Eli Lilly, Pfizer, Rani, Revolo, Sanofi, Scipher, SciRom, SetPoint, and Tremeau; stock options from Canfite, Inmedex, and Scipher, all unrelated to this work. Dr. Shadick has received research grants from AbbVie, Amgen, Aqtual, Bristol Myers Squibb, Eli Lilly, and Mallinckrodt unrelated to this work. Dr. Doyle has received research support from Bristol Myers Squibb; consulting fees from Boehringer Ingelheim and L.E.K. consulting; speaking fees and travel support from Aura; and has been part of a clinical trial funded by Genentech, unrelated to this work. Dr. Sparks has received research support from Bristol Myers Squibb and performed consultancy for AbbVie, Amgen, Boehringer Ingelheim, Bristol Myers Squibb, Gilead, Inova Diagnostics, Janssen, Optum, and Pfizer unrelated to this work.
Figures
Comment in
-
Predicting rheumatoid arthritis-associated interstitial lung disease: filling the void.Lancet Rheumatol. 2023 Feb;5(2):e61-e63. doi: 10.1016/S2665-9913(23)00008-5. Lancet Rheumatol. 2023. PMID: 38251539 No abstract available.
References
-
- Hyldgaard C, Hilberg O, Pedersen AB, et al. A population-based cohort study of rheumatoid arthritis-associated interstitial lung disease: comorbidity and mortality. Ann Rheum Dis 2017; 76(10): 1700–6. - PubMed
Grants and funding
- R01 AR077607/AR/NIAMS NIH HHS/United States
- R01 HL130974/HL/NHLBI NIH HHS/United States
- P30 AR070253/AR/NIAMS NIH HHS/United States
- R01 AR080659/AR/NIAMS NIH HHS/United States
- T32 AR007530/AR/NIAMS NIH HHS/United States
- R01 HL111024/HL/NHLBI NIH HHS/United States
- R01 HL135142/HL/NHLBI NIH HHS/United States
- K23 AR069688/AR/NIAMS NIH HHS/United States
- L30 AR066953/AR/NIAMS NIH HHS/United States
- R03 AR075886/AR/NIAMS NIH HHS/United States
- P30 AR072577/AR/NIAMS NIH HHS/United States
- R01 HL155522/HL/NHLBI NIH HHS/United States
- R01 CA203636/CA/NCI NIH HHS/United States
- U01 CA209414/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources