

Sentinel Node Procedure to Select Clinically Localized Prostate Cancer Patients with Occult Nodal Metastases for Whole Pelvis Radiotherapy
- PMID: 36874598
- PMCID: PMC9975002
- DOI: 10.1016/j.euros.2022.12.011
Sentinel Node Procedure to Select Clinically Localized Prostate Cancer Patients with Occult Nodal Metastases for Whole Pelvis Radiotherapy
Abstract
Background: Accurate identification of men who harbor nodal metastases is necessary to select patients who most likely benefit from whole pelvis radiotherapy (WPRT). Limited sensitivity of diagnostic imaging approaches for the detection of nodal micrometastases has led to the exploration of the sentinel lymph node biopsy (SLNB).
Objective: To evaluate whether SLNB can be used as a tool to select pathologically node-positive patients who likely benefit from WPRT.
Design setting and participants: We included 528 clinically node-negative primary prostate cancer (PCa) patients with an estimated nodal risk of >5% treated between 2007 and 2018.
Intervention: A total of 267 patients were directly treated with prostate-only radiotherapy (PORT; non-SLNB group), while 261 patients underwent SLNB to remove lymph nodes directly draining from the primary tumor prior to radiotherapy (SLNB group); pN0 patients were treated with PORT, while pN1 patients were offered WPRT.
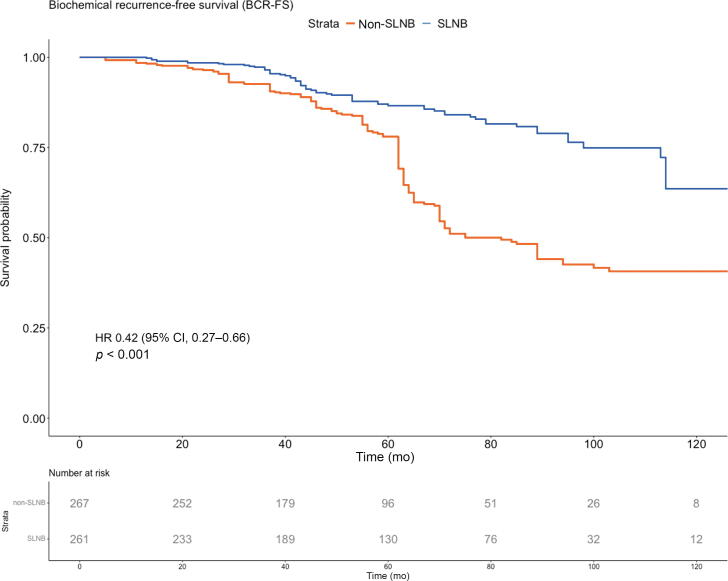
Outcome measurements and statistical analysis: Biochemical recurrence-free survival (BCRFS) and radiological recurrence-free survival (RRFS) were compared using propensity score weighted (PSW) Cox proportional hazard models.
Results and limitations: The median follow-up was 71 mo. Occult nodal metastases were found in 97 (37%) SLNB patients (median metastasis size: 2 mm). Adjusted 7-yr BCRFS rates were 81% (95% confidence interval [CI] 77-86%) in the SLNB group and 49% (95% CI 43-56%) in the non-SLNB group. The corresponding adjusted 7-yr RRFS rates were 83% (95% CI 78-87%) and 52% (95% CI 46-59%), respectively. In the PSW multivariable Cox regression analysis, SLNB was associated with improved BCRFS (hazard ratio [HR] 0.38, 95% CI 0.25-0.59, p < 0.001) and RRFS (HR 0.44, 95% CI 0.28-0.69, p < 0.001). Limitations include the bias inherent to the study's retrospective nature.
Conclusions: SLNB-based selection of pN1 PCa patients for WPRT was associated with significantly improved BCRFS and RRFS compared with (conventional) imaging-based PORT.
Patient summary: Sentinel node biopsy can be used to select patients who will benefit from the addition of pelvis radiotherapy. This strategy results in a longer duration of prostate-specific antigen control and a lower risk of radiological recurrence.
Keywords: Prostate cancer; Prostate-only radiotherapy; Sentinel lymph node procedure; Whole pelvis radiotherapy.
© 2023 The Author(s).
Figures






Comment in
-
Detecting lymph node metastases for personalized radiotherapy in patients with prostate cancer.Nat Rev Urol. 2023 Apr;20(4):197. doi: 10.1038/s41585-023-00753-y. Nat Rev Urol. 2023. PMID: 36899178 No abstract available.
References
-
- Mottet N., van den Bergh R.C.N., Briers E., et al. EAU-EANM-ESTRO-ESUR-SIOG guidelines on prostate cancer—2020 update. Part 1: screening, diagnosis, and local treatment with curative intent. Eur Urol. 2021;79:243–262. - PubMed
-
- Van Hemelryk A., De Meerleer G., Ost P., et al. The outcome for patients with pathologic node-positive prostate cancer treated with intensity modulated radiation therapy and androgen deprivation therapy: a case-matched analysis of pN1 and pN0 patients. Int J Radiat Oncol. 2016;96:323–332. - PubMed
-
- Poelaert F., Fonteyne V., Ost P., et al. Whole pelvis radiotherapy for pathological node-positive prostate cancer. Strahlentherapie Und Onkol. 2017;193:444–451. - PubMed
-
- Murthy V., Maitre P., Kannan S., et al. Prostate-only versus whole-pelvic radiation therapy in high-risk and very high-risk prostate cancer (POP-RT): outcomes from phase III randomized controlled trial. J Clin Oncol. 2021;39:1234–1242. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
