

Bacterial and viral infections among adults hospitalized with COVID-19, COVID-NET, 14 states, March 2020-April 2022
- PMID: 36875205
- PMCID: PMC9981874
- DOI: 10.1111/irv.13107
Bacterial and viral infections among adults hospitalized with COVID-19, COVID-NET, 14 states, March 2020-April 2022
Abstract
Background: Bacterial and viral infections can occur with SARS-CoV-2 infection, but prevalence, risk factors, and associated clinical outcomes are not fully understood.
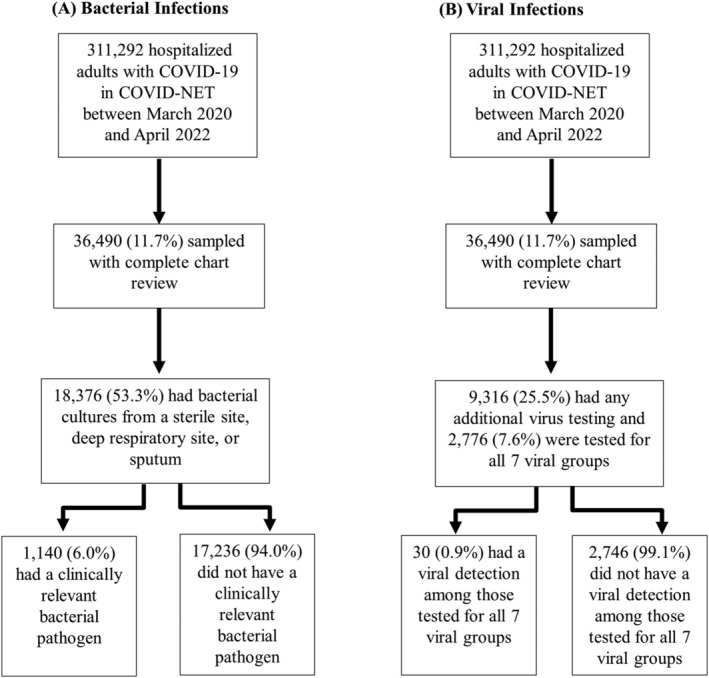
Methods: We used the Coronavirus Disease 2019-Associated Hospitalization Surveillance Network (COVID-NET), a population-based surveillance system, to investigate the occurrence of bacterial and viral infections among hospitalized adults with laboratory-confirmed SARS-CoV-2 infection between March 2020 and April 2022. Clinician-driven testing for bacterial pathogens from sputum, deep respiratory, and sterile sites were included. The demographic and clinical features of those with and without bacterial infections were compared. We also describe the prevalence of viral pathogens including respiratory syncytial virus, rhinovirus/enterovirus, influenza, adenovirus, human metapneumovirus, parainfluenza viruses, and non-SARS-CoV-2 endemic coronaviruses.
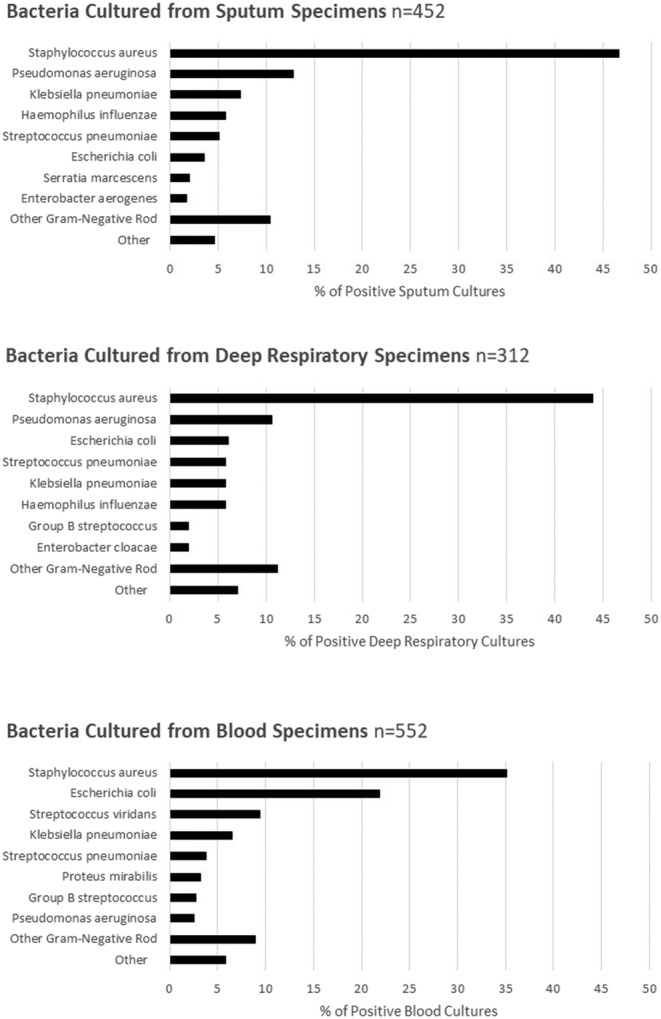
Results: Among 36 490 hospitalized adults with COVID-19, 53.3% had bacterial cultures taken within 7 days of admission and 6.0% of these had a clinically relevant bacterial pathogen. After adjustment for demographic factors and co-morbidities, bacterial infections in patients with COVID-19 within 7 days of admission were associated with an adjusted relative risk of death 2.3 times that of patients with negative bacterial testing. Staphylococcus aureus and Gram-negative rods were the most frequently isolated bacterial pathogens. Among hospitalized adults with COVID-19, 2766 (7.6%) were tested for seven virus groups. A non-SARS-CoV-2 virus was identified in 0.9% of tested patients.
Conclusions: Among patients with clinician-driven testing, 6.0% of adults hospitalized with COVID-19 were identified to have bacterial coinfections and 0.9% were identified to have viral coinfections; identification of a bacterial coinfection within 7 days of admission was associated with increased mortality.
Keywords: COVID‐19; COVID‐NET; SARS‐CoV‐2; bacterial coinfection; viral coinfection.
© 2023 The Authors. Influenza and Other Respiratory Viruses published by John Wiley & Sons Ltd. This article has been contributed to by U.S. Government employees and their work is in the public domain in the USA.
Conflict of interest statement
Ms. Leegwater and Ms. Reeg report grants from Michigan Department of Health and Human Services during the conduct of the study. Dr. Anderson reports grants from Pfizer, Merck, PaxVax, Micron, Sanofi‐Pasteur, Janssen, MedImmune, and GSK. Dr. Anderson reports personal fees from Sanofi‐Pasteur, Pfizer, Medscape, Kentucky Bioprocessing, Inc, Sanofi‐Pasteur, Janssen, GSK, WCG and ACI Clinical, and Moderna outside the submitted work. His institution has also received funding from NIH to conduct clinical trials of Moderna and Janssen COVID‐19 vaccines. Mr. Weigel reports grants from CDC/CSTE Cooperative Agreement, during the conduct of the study and grants from CDC/CSTE outside the submitted work. Mr. Teno reports grants from CDC/CSTE Cooperative Agreement during the conduct of the study and grants from CDC/CSTE outside the submitted work. Mrs. Billing reports grants from Council of State and Territorial Epidemiologists (CSTE) during the conduct of the study and grants from Centers for Disease Control and Prevention (CDC) outside the submitted work. Mr. Meek reports grants from CDC during the conduct of the study. Dr. Schaffner reports grants from CDC during the conduct of the study. Dr. Sutton reports grants from CDC Emerging Infections Program during the conduct of the study. Dr. Talbot reports grants from Centers for Disease Control and Prevention, during the conduct of the study. Ms. Yousey‐Hindes reports grants from CDC during the conduct of the study.
Figures
References
-
- Russell K, Fowlkes A, Lynfield R, et al. Viral and bacterial co‐detections in influenza‐positive patients hospitalized with severe acute respiratory illness—Minnesota, 2013–2015. Open Forum Infect Dis. 2016;3(suppl_1):1754. doi:10.1093/ofid/ofw194.134 - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
