

Clinical characteristics and outcomes of immunocompromised patients with severe community-acquired pneumonia: A single-center retrospective cohort study
- PMID: 36875372
- PMCID: PMC9975557
- DOI: 10.3389/fpubh.2023.1070581
Clinical characteristics and outcomes of immunocompromised patients with severe community-acquired pneumonia: A single-center retrospective cohort study
Abstract
Background: Immunocompromised patients with severe community-acquired pneumonia (SCAP) warrant special attention because they comprise a growing proportion of patients and tend to have poor clinical outcomes. The objective of this study was to compare the characteristics and outcomes of immunocompromised and immunocompetent patients with SCAP, and to investigate the risk factors for mortality in these patients.
Methods: We conducted retrospective observational cohort study of patients aged ≥18 years admitted to the intensive care unit (ICU) of an academic tertiary hospital with SCAP between January 2017 and December 2019 and compared the clinical characteristics and outcomes of immunocompromised and immunocompetent patients.
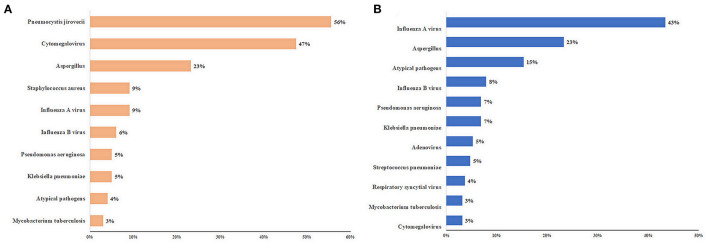
Results: Among the 393 patients, 119 (30.3%) were immunocompromised. Corticosteroid (51.2%) and immunosuppressive drug (23.5%) therapies were the most common causes. Compared to immunocompetent patients, immunocompromised patients had a higher frequency of polymicrobial infection (56.6 vs. 27.5%, P < 0.001), early mortality (within 7 days) (26.1 vs. 13.1%, P = 0.002), and ICU mortality (49.6 vs. 37.6%, P = 0.027). The pathogen distributions differed between immunocompromised and immunocompetent patients. Among immunocompromised patients, Pneumocystis jirovecii and cytomegalovirus were the most common pathogens. Immunocompromised status (OR: 2.043, 95% CI: 1.114-3.748, P = 0.021) was an independent risk factor for ICU mortality. Independent risk factors for ICU mortality in immunocompromised patients included age ≥ 65 years (odds ratio [OR]: 9.098, 95% confidence interval [CI]: 1.472-56.234, P = 0.018), SOFA score [OR: 1.338, 95% CI: 1.048-1.708, P = 0.019), lymphocyte count < 0.8 × 109/L (OR: 6.640, 95% CI: 1.463-30.141, P = 0.014), D-dimer level (OR: 1.160, 95% CI: 1.013-1.329, P = 0.032), FiO2 > 0.7 (OR: 10.228, 95% CI: 1.992-52.531, P = 0.005), and lactate level (OR: 4.849, 95% CI: 1.701-13.825, P = 0.003).
Conclusions: Immunocompromised patients with SCAP have distinct clinical characteristics and risk factors that should be considered in their clinical evaluation and management.
Keywords: clinical characteristics; community-acquired pneumonia; immunocompromised status; intensive care unit; risk factor.
Copyright © 2023 Wu, Sun, Cai, Zhai, Liu, Gu, Zhou and Zhan.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Clinical characteristics and risk factors associated with mortality in patients with severe community-acquired pneumonia and type 2 diabetes mellitus.Crit Care. 2021 Dec 7;25(1):419. doi: 10.1186/s13054-021-03841-w. Crit Care. 2021. PMID: 34876193 Free PMC article.
-
[Etiology of severe community-acquired pneumonia in immunocompromised patients].Zhonghua Jie He He Hu Xi Za Zhi. 2021 Oct 12;44(10):892-896. doi: 10.3760/cma.j.cn112147-20210131-00087. Zhonghua Jie He He Hu Xi Za Zhi. 2021. PMID: 34565116 Chinese.
-
[Timing of sequential noninvasive mechanical ventilation following early extubation in aged patients with severe community-acquired pneumonia].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020 Mar;32(3):324-329. doi: 10.3760/cma.j.cn121430-20191224-00072. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020. PMID: 32385997 Chinese.
-
Metagenomic Next-Generation Sequencing for Pathogenic Diagnosis and Antibiotic Management of Severe Community-Acquired Pneumonia in Immunocompromised Adults.Front Cell Infect Microbiol. 2021 Jun 1;11:661589. doi: 10.3389/fcimb.2021.661589. eCollection 2021. Front Cell Infect Microbiol. 2021. PMID: 34141628 Free PMC article.
-
Ten Issues for Updating in Community-Acquired Pneumonia: An Expert Review.J Clin Med. 2023 Oct 30;12(21):6864. doi: 10.3390/jcm12216864. J Clin Med. 2023. PMID: 37959328 Free PMC article. Review.
Cited by
-
Diagnostic performance of Pneumonia multiplex PCR in critically ill immunocompromised patients.Crit Care. 2025 Jul 17;29(1):310. doi: 10.1186/s13054-025-05528-y. Crit Care. 2025. PMID: 40676679 Free PMC article.
-
Utility of Metagenomic Next-Generation Sequencing for Diagnosis of Infectious Diseases in Critically Ill Immunocompromised Pediatric Patients.Infect Drug Resist. 2024 Aug 16;17:3579-3591. doi: 10.2147/IDR.S472129. eCollection 2024. Infect Drug Resist. 2024. PMID: 39165848 Free PMC article.
-
Factors based on Cox regression modeling to analyze the prognostic impact of fiberoptic bronchoscopic bronchoalveolar lavage on children with severe pneumonia.Am J Transl Res. 2024 Dec 15;16(12):7645-7655. doi: 10.62347/OGZD3131. eCollection 2024. Am J Transl Res. 2024. PMID: 39822555 Free PMC article.
-
A Case of Severe Community-Acquired Pneumonia Caused by Coinfection of Five Pathogens.Infect Drug Resist. 2025 Mar 19;18:1515-1519. doi: 10.2147/IDR.S483156. eCollection 2025. Infect Drug Resist. 2025. PMID: 40123706 Free PMC article.
-
What intensivists need to know about cytomegalovirus infection in immunocompromised ICU patients.Intensive Care Med. 2025 Jan;51(1):39-61. doi: 10.1007/s00134-024-07737-5. Epub 2025 Jan 7. Intensive Care Med. 2025. PMID: 39774866 Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical