

Hemodynamic Effects of a High-Frequency Oscillatory Ventilation Open-Lung Strategy in Critically Ill Children With Acquired or Congenital Cardiac Disease
- PMID: 36877029
- PMCID: PMC10226461
- DOI: 10.1097/PCC.0000000000003211
Hemodynamic Effects of a High-Frequency Oscillatory Ventilation Open-Lung Strategy in Critically Ill Children With Acquired or Congenital Cardiac Disease
Abstract
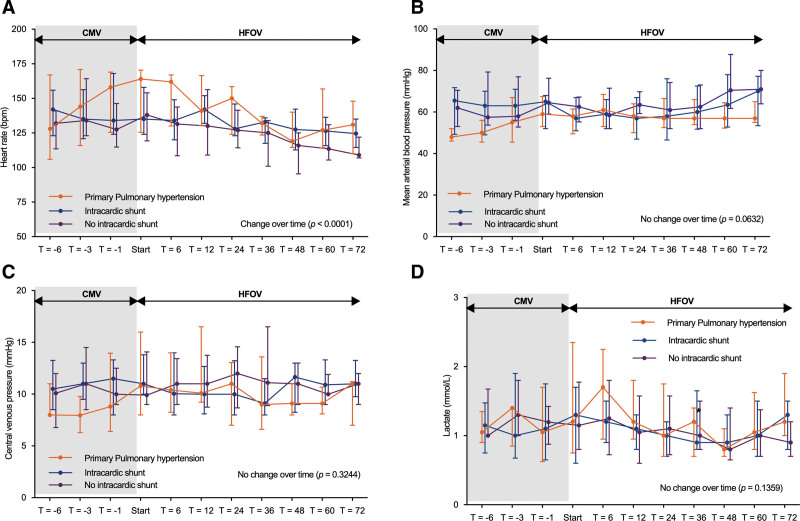
Objectives: To study the hemodynamic consequences of an open-lung high-frequency oscillatory ventilation (HFOV) strategy in patients with an underlying cardiac anomaly with or without intracardiac shunt or primary pulmonary hypertension with severe lung injury.
Design: Secondary analysis of prospectively collected data.
Setting: Medical-surgical PICU.
Patients: Children less than 18 years old with cardiac anomalies (± intracardiac shunt) or primary pulmonary hypertension.
Interventions: None.
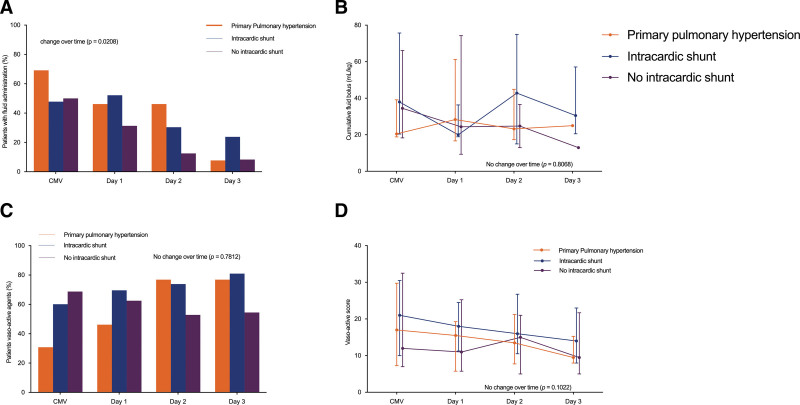
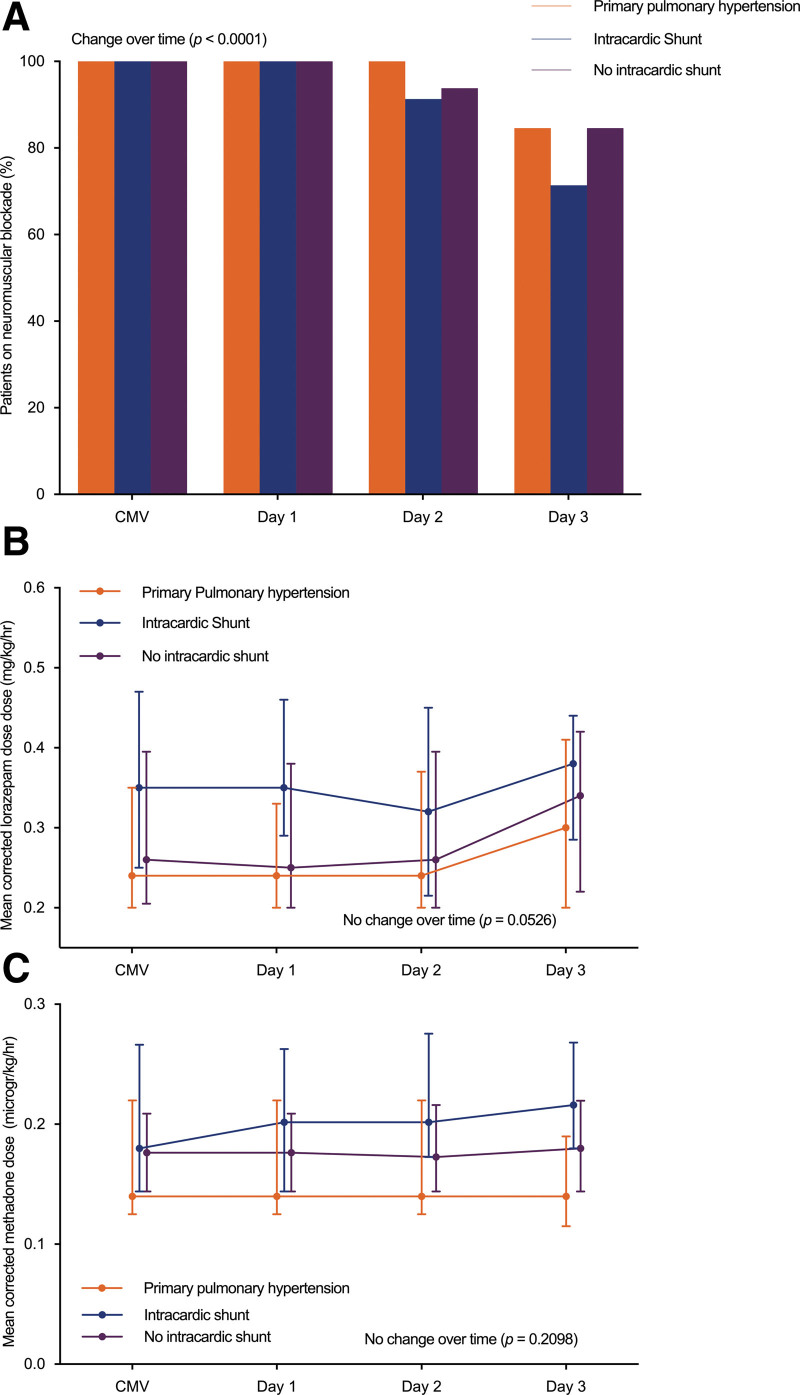
Measurements and main results: Data from 52 subjects were analyzed, of whom 39 of 52 with cardiac anomaly (23/39 with intracardiac shunt) and 13 of 52 with primary pulmonary hypertension. Fourteen patients were admitted postoperatively, and 26 patients were admitted with acute respiratory failure. Five subjects (9.6%) were canulated for ECMO (of whom four for worsening respiratory status). Ten patients (19.2%) died during PICU stay. Median conventional mechanical ventilation settings prior to HFOV were peak inspiratory pressure 30 cm H 2 O (27-33 cm H 2 O), positive end-expiratory pressure 8 cm H 2 O (6-10 cm H 2 O), and F io2 0.72 (0.56-0.94). After transitioning to HFOV, there was no negative effect on mean arterial blood pressure, central venous pressure, or arterial lactate. Heart rate decreased significantly over time ( p < 0.0001), without group differences. The percentage of subjects receiving a fluid bolus decreased over time ( p = 0.003), especially in those with primary pulmonary hypertension ( p = 0.0155) and without intracardiac shunt ( p = 0.0328). There were no significant differences in the cumulative number of daily boluses over time. Vasoactive Infusion Score did not increase over time. Pa co2 decreased ( p < 0.0002) and arterial pH significantly improved ( p < 0.0001) over time in the whole cohort. Neuromuscular blocking agents were used in all subjects switched to HFOV. Daily cumulative sedative doses were unchanged, and no clinically apparent barotrauma was found.
Conclusions: No negative hemodynamic consequences occurred with an individualized, physiology-based open-lung HFOV approach in patients with cardiac anomalies or primary pulmonary hypertension suffering from severe lung injury.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies.
Conflict of interest statement
Dr. Curley’s institution received funding from the National Heart, Lung, and Blood Institute and the National Institute of Child Health and Human Development; she received support for article research from the National Institutes of Health. Dr. Cheifetz received funding from Philips, Medtronic, Tim Peters and Co, and UptoDate. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Similar articles
-
Effect of early intervention of high-frequency oscillatory ventilation on the outcome in pediatric acute respiratory distress syndrome.Bratisl Lek Listy. 2000;101(1):8-13. Bratisl Lek Listy. 2000. PMID: 10824405
-
Feasibility of an alternative, physiologic, individualized open-lung approach to high-frequency oscillatory ventilation in children.Ann Intensive Care. 2019 Jan 18;9(1):9. doi: 10.1186/s13613-019-0492-0. Ann Intensive Care. 2019. PMID: 30659380 Free PMC article.
-
[Effects of high frequency oscillatory ventilation combined with incremental positive end-expiratory pressure on respiratory and circulatory functions of dogs with inhalation injury].Zhonghua Shao Shang Za Zhi. 2013 Jun;29(3):255-60. Zhonghua Shao Shang Za Zhi. 2013. PMID: 24059950 Chinese.
-
High-frequency oscillatory ventilation for acute respiratory distress syndrome in adult patients.Crit Care Med. 2003 Apr;31(4 Suppl):S317-23. doi: 10.1097/01.CCM.0000057910.50618.EB. Crit Care Med. 2003. PMID: 12682459 Review.
-
Elective high-frequency oscillatory ventilation versus conventional ventilation for acute pulmonary dysfunction in preterm infants.Neonatology. 2013;103(1):7-8; discussion 8-9. doi: 10.1159/000338553. Epub 2012 Aug 30. Neonatology. 2013. PMID: 23037971 Review.
Cited by
-
Pediatric cardiac patients with pulmonary hemorrhage supported on ECMO: An ELSO registry study.J Extra Corpor Technol. 2025 Mar;57(1):2-8. doi: 10.1051/ject/2024038. Epub 2025 Mar 7. J Extra Corpor Technol. 2025. PMID: 40053851 Free PMC article.
References
-
- Healy F, Hanna BD, Zinman R: Pulmonary complications of congenital heart disease. Paediatr Respir Rev. 2012; 13:10–15 - PubMed
-
- Johnson BN, Fierro JL, Panitch HB: Pulmonary manifestations of congenital heart disease in children. Pediatr Clin North Am. 2021; 68:25–40 - PubMed
-
- Imai Y, Slutsky AS: High-frequency oscillatory ventilation and ventilator-induced lung injury. Crit Care Med. 2005; 33:S129–S134 - PubMed
-
- Imai Y, Nakagawa S, Ito Y, et al. : Comparison of lung protection strategies using conventional and high-frequency oscillatory ventilation. J Appl Physiol (1985). 2001; 91:1836–1844 - PubMed
-
- Carney D, DiRocco J, Nieman G: Dynamic alveolar mechanics and ventilator-induced lung injury. Crit Care Med. 2005; 33:S122–S128 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
