

Coordinated Care to Optimize Cardiovascular Preventive Therapies in Type 2 Diabetes: A Randomized Clinical Trial
- PMID: 36877177
- PMCID: PMC9989955
- DOI: 10.1001/jama.2023.2854
Coordinated Care to Optimize Cardiovascular Preventive Therapies in Type 2 Diabetes: A Randomized Clinical Trial
Abstract
Importance: Evidence-based therapies to reduce atherosclerotic cardiovascular disease risk in adults with type 2 diabetes are underused in clinical practice.
Objective: To assess the effect of a coordinated, multifaceted intervention of assessment, education, and feedback vs usual care on the proportion of adults with type 2 diabetes and atherosclerotic cardiovascular disease prescribed all 3 groups of recommended, evidence-based therapies (high-intensity statins, angiotensin-converting enzyme inhibitors [ACEIs] or angiotensin receptor blockers [ARBs], and sodium-glucose cotransporter 2 [SGLT2] inhibitors and/or glucagon-like peptide 1 receptor agonists [GLP-1RAs]).
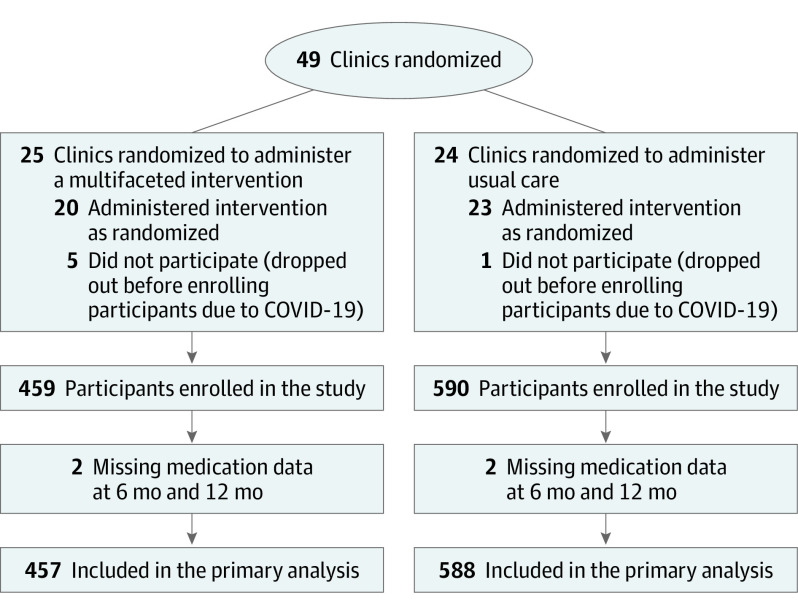
Design, setting, and participants: Cluster randomized clinical trial with 43 US cardiology clinics recruiting participants from July 2019 through May 2022 and follow-up through December 2022. The participants were adults with type 2 diabetes and atherosclerotic cardiovascular disease not already taking all 3 groups of evidence-based therapies.
Interventions: Assessing local barriers, developing care pathways, coordinating care, educating clinicians, reporting data back to the clinics, and providing tools for participants (n = 459) vs usual care per practice guidelines (n = 590).
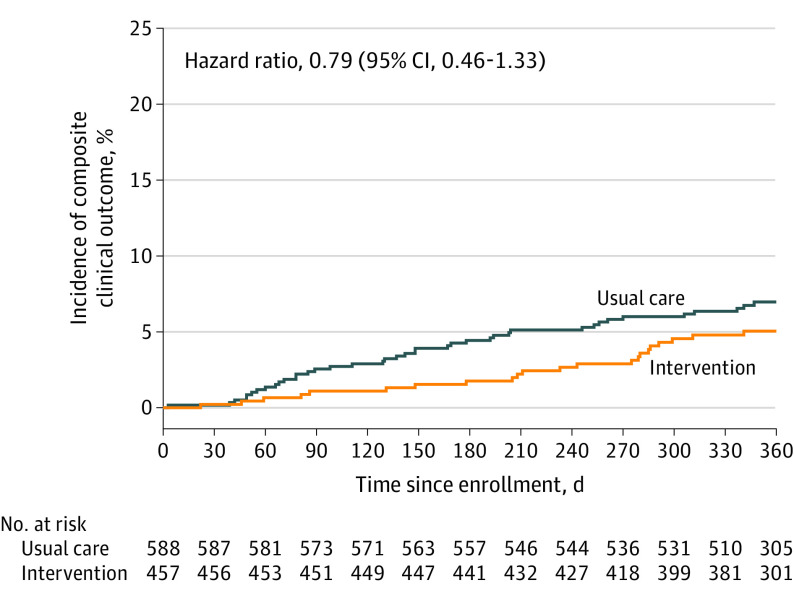
Main outcomes and measures: The primary outcome was the proportion of participants prescribed all 3 groups of recommended therapies at 6 to 12 months after enrollment. The secondary outcomes included changes in atherosclerotic cardiovascular disease risk factors and a composite outcome of all-cause death or hospitalization for myocardial infarction, stroke, decompensated heart failure, or urgent revascularization (the trial was not powered to show these differences).
Results: Of 1049 participants enrolled (459 at 20 intervention clinics and 590 at 23 usual care clinics), the median age was 70 years and there were 338 women (32.2%), 173 Black participants (16.5%), and 90 Hispanic participants (8.6%). At the last follow-up visit (12 months for 97.3% of participants), those in the intervention group were more likely to be prescribed all 3 therapies (173/457 [37.9%]) vs the usual care group (85/588 [14.5%]), which is a difference of 23.4% (adjusted odds ratio [OR], 4.38 [95% CI, 2.49 to 7.71]; P < .001) and were more likely to be prescribed each of the 3 therapies (change from baseline in high-intensity statins from 66.5% to 70.7% for intervention vs from 58.2% to 56.8% for usual care [adjusted OR, 1.73; 95% CI, 1.06-2.83]; ACEIs or ARBs: from 75.1% to 81.4% for intervention vs from 69.6% to 68.4% for usual care [adjusted OR, 1.82; 95% CI, 1.14-2.91]; SGLT2 inhibitors and/or GLP-1RAs: from 12.3% to 60.4% for intervention vs from 14.5% to 35.5% for usual care [adjusted OR, 3.11; 95% CI, 2.08-4.64]). The intervention was not associated with changes in atherosclerotic cardiovascular disease risk factors. The composite secondary outcome occurred in 23 of 457 participants (5%) in the intervention group vs 40 of 588 participants (6.8%) in the usual care group (adjusted hazard ratio, 0.79 [95% CI, 0.46 to 1.33]).
Conclusions and relevance: A coordinated, multifaceted intervention increased prescription of 3 groups of evidence-based therapies in adults with type 2 diabetes and atherosclerotic cardiovascular disease.
Trial registration: ClinicalTrials.gov Identifier: NCT03936660.
Conflict of interest statement
Figures

Comment in
-
Coordinated Care for Optimization of Cardiovascular Preventive Therapies in Patients With Diabetes.JAMA. 2023 Aug 22;330(8):771. doi: 10.1001/jama.2023.11538. JAMA. 2023. PMID: 37606678 No abstract available.
References
-
- US Centers for Disease Control and Prevention . National Diabetes Statistics Report: estimates of diabetes and its burden in the United States. Accessed June 20, 2022. https://www.cdc.gov/diabetes/data/statistics-report/index.html
-
- Sarwar N, Gao P, Seshasai SR, et al. ; Emerging Risk Factors Collaboration . Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: a collaborative meta-analysis of 102 prospective studies. Lancet. 2010;375(9733):2215-2222. Published correction appears in Lancet. 2010;376(9745):958. doi: 10.1016/S0140-6736(10)60484-9 - DOI - PMC - PubMed
-
- Kearney PM, Blackwell L, Collins R, et al. ; Cholesterol Treatment Trialists’ (CTT) Collaborators . Efficacy of cholesterol-lowering therapy in 18,686 people with diabetes in 14 randomised trials of statins: a meta-analysis. Lancet. 2008;371(9607):117-125. doi: 10.1016/S0140-6736(08)60104-X - DOI - PubMed
-
- Foulquier S, Böhm M, Schmieder R, et al. Impact of telmisartan on cardiovascular outcome in hypertensive patients at high risk: a Telmisartan Randomised AssessmeNt Study in ACE iNtolerant subjects with cardiovascular Disease subanalysis. J Hypertens. 2014;32(6):1334-1341. doi: 10.1097/HJH.0000000000000154 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
