

Effect of Routine Invasive vs Conservative Strategy in Older Adults With Frailty and Non-ST-Segment Elevation Acute Myocardial Infarction: A Randomized Clinical Trial
- PMID: 36877502
- PMCID: PMC9989957
- DOI: 10.1001/jamainternmed.2023.0047
Effect of Routine Invasive vs Conservative Strategy in Older Adults With Frailty and Non-ST-Segment Elevation Acute Myocardial Infarction: A Randomized Clinical Trial
Abstract
Importance: To our knowledge, no randomized clinical trial has compared the invasive and conservative strategies in frail, older patients with non-ST-segment elevation acute myocardial infarction (NSTEMI).
Objective: To compare outcomes of invasive and conservative strategies in frail, older patients with NSTEMI at 1 year.
Design, setting, and participants: This multicenter randomized clinical trial was conducted at 13 Spanish hospitals between July 7, 2017, and January 9, 2021, and included 167 older adult (≥70 years) patients with frailty (Clinical Frailty Scale score ≥4) and NSTEMI. Data analysis was performed from April 2022 to June 2022.
Interventions: Patients were randomized to routine invasive (coronary angiography and revascularization if feasible; n = 84) or conservative (medical treatment with coronary angiography for recurrent ischemia; n = 83) strategy.
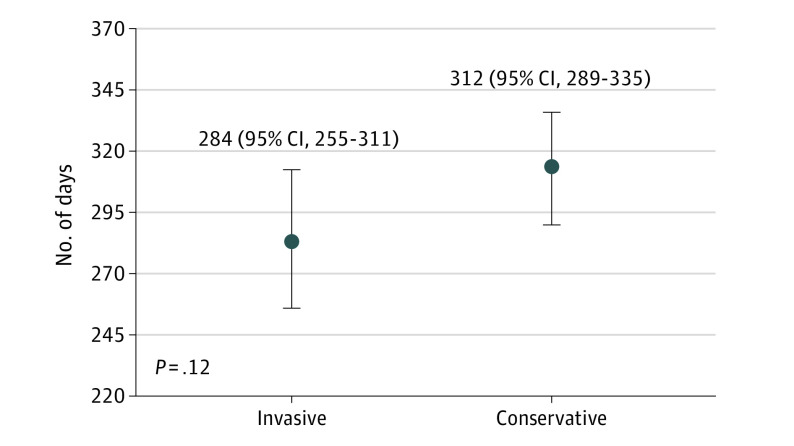
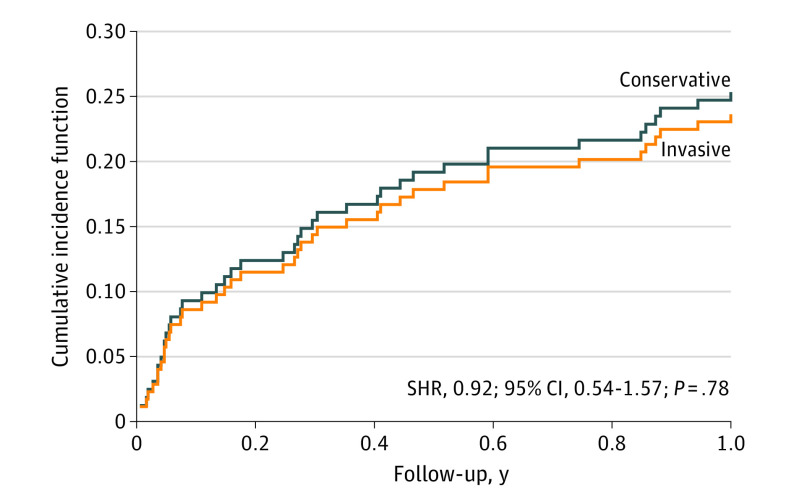
Main outcomes and measures: The primary end point was the number of days alive and out of the hospital (DAOH) from discharge to 1 year. The coprimary end point was the composite of cardiac death, reinfarction, or postdischarge revascularization.
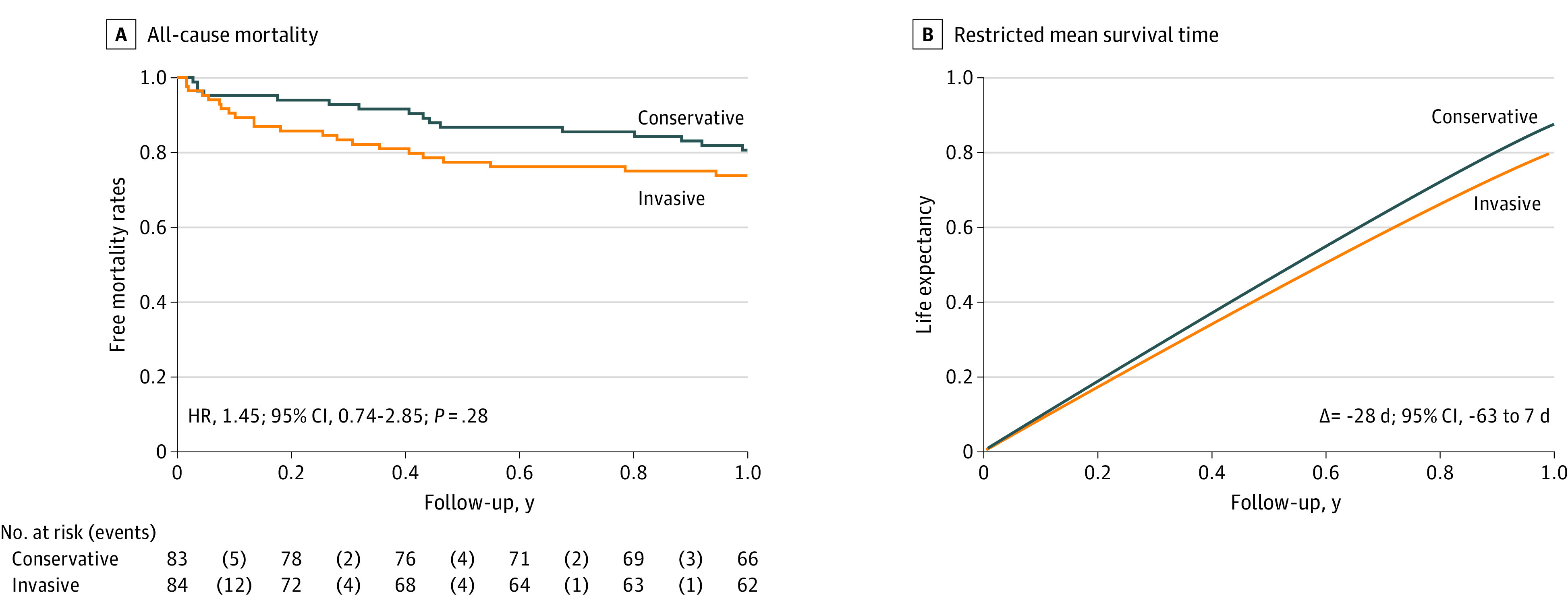
Results: The study was prematurely stopped due to the COVID-19 pandemic when 95% of the calculated sample size had been enrolled. Among the 167 patients included, the mean (SD) age was 86 (5) years, and mean (SD) Clinical Frailty Scale score was 5 (1). While not statistically different, DAOH were about 1 month (28 days; 95% CI, -7 to 62) greater for patients managed conservatively (312 days; 95% CI, 289 to 335) vs patients managed invasively (284 days; 95% CI, 255 to 311; P = .12). A sensitivity analysis stratified by sex did not show differences. In addition, we found no differences in all-cause mortality (hazard ratio, 1.45; 95% CI, 0.74-2.85; P = .28). There was a 28-day shorter survival in the invasive vs conservatively managed group (95% CI, -63 to 7 days; restricted mean survival time analysis). Noncardiac reasons accounted for 56% of the readmissions. There were no differences in the number of readmissions or days spent in the hospital after discharge between groups. Neither were there differences in the coprimary end point of ischemic cardiac events (subdistribution hazard ratio, 0.92; 95% CI, 0.54-1.57; P = .78).
Conclusions and relevance: In this randomized clinical trial of NSTEMI in frail older patients, there was no benefit to a routine invasive strategy in DAOH during the first year. Based on these findings, a policy of medical management and watchful observation is recommended for older patients with frailty and NSTEMI.
Trial registration: ClinicalTrials.gov Identifier: NCT03208153.
Conflict of interest statement
Figures
Comment in
-
Importance of Designing Trials for Older Adults With Complex Medical Conditions.JAMA Intern Med. 2023 May 1;183(5):415-416. doi: 10.1001/jamainternmed.2023.0046. JAMA Intern Med. 2023. PMID: 36877494 No abstract available.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
