

Effects of COVID-19 Acute Respiratory Distress Syndrome Intensive Care Unit Survivor Telemedicine Clinic on Patient Readmission, Pain Perception, and Self-Assessed Health Scores: Randomized, Prospective, Single-Center, Exploratory Study
- PMID: 36877802
- PMCID: PMC10036111
- DOI: 10.2196/43759
Effects of COVID-19 Acute Respiratory Distress Syndrome Intensive Care Unit Survivor Telemedicine Clinic on Patient Readmission, Pain Perception, and Self-Assessed Health Scores: Randomized, Prospective, Single-Center, Exploratory Study
Abstract
Background: Post-intensive care syndrome (PICS) affects up to 50% of intensive care unit (ICU) survivors, leading to long-term neurocognitive, psychosocial, and physical impairments. Approximately 80% of COVID-19 pneumonia ICU patients are at elevated risk for developing acute respiratory distress syndrome (ARDS). Survivors of COVID-19 ARDS are at high risk of unanticipated health care utilization postdischarge. This patient group commonly has increased readmission rates, long-term decreased mobility, and poorer outcomes. Most multidisciplinary post-ICU clinics for ICU survivors are in large urban academic medical centers providing in-person consultation. Data are lacking on the feasibility of providing telemedicine post-ICU care for COVID-19 ARDS survivors.
Objective: We explored the feasibility of instituting a COVID-19 ARDS ICU survivor telemedicine clinic and examined its effect on health care utilization post-hospital discharge.
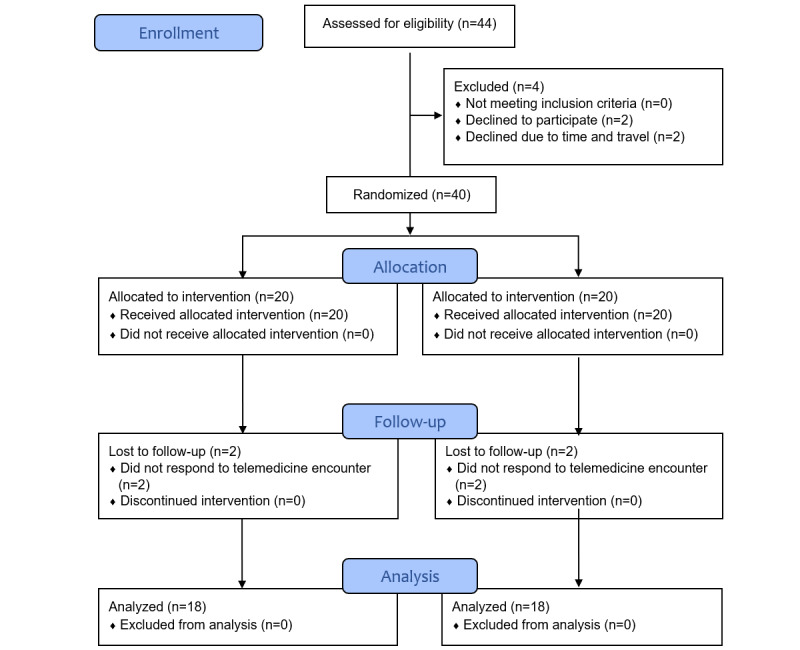
Methods: This randomized, unblinded, single-center, parallel-group, exploratory study was conducted at a rural, academic medical center. Study group (SG) participants underwent a telemedicine visit within 14 days of discharge, during which a 6-minute walk test (6MWT), EuroQoL 5-Dimension (EQ-5D) questionnaire, and vital signs logs were reviewed by an intensivist. Additional appointments were arranged as needed based on the outcome of this review and tests. The control group (CG) underwent a telemedicine visit within 6 weeks of discharge and completed the EQ-5D questionnaire; additional care was provided as needed based on findings in this telemedicine visit.
Results: Both SG (n=20) and CG (n=20) participants had similar baseline characteristics and dropout rate (10%). Among SG participants, 72% (13/18) agreed to pulmonary clinic follow-up, compared with 50% (9/18) of CG participants (P=.31). Unanticipated visits to the emergency department occurred for 11% (2/18) of the SG compared with 6% (1/18) of the CG (>.99). The rate of pain or discomfort was 67% (12/18) in the SG compared with 61% (11/18) in the CG (P=.72). The anxiety or depression rate was 72% (13/18) in the SG versus 61% (11/18; P=.59) in the CG. Participants' mean self-assessed health rating scores were 73.9 (SD 16.1) in the SG compared with 70.6 (SD 20.9) in the CG (P=.59). Both primary care physicians (PCPs) and participants in the SG perceived the telemedicine clinic as a favorable model for postdischarge critical illness follow-up in an open-ended questionnaire regarding care.
Conclusions: This exploratory study found no statistically significant results in reducing health care utilization postdischarge and health-related quality of life. However, PCPs and patients perceived telemedicine as a feasible and favorable model for postdischarge care among COVID-19 ICU survivors to facilitate expedited subspecialty assessment, decrease unanticipated postdischarge health care utilization, and reduce PICS. Further investigation is warranted to determine the feasibility of incorporating telemedicine-based post-hospitalization follow-up for all medical ICU survivors that may show improvement in health care utilization in a larger population.
Keywords: COVID-19 pneumonia; acute respiratory distress syndrome; aftercare; critical care; survivor; telemedicine.
©Bathmapriya Balakrishnan, Lucas Hamrick, Ariful Alam, Jesse Thompson. Originally published in JMIR Formative Research (https://formative.jmir.org), 22.03.2023.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
Similar articles
-
Implementing an intensive care unit (ICU) diary program at a large academic medical center: Results from a randomized control trial evaluating psychological morbidity associated with critical illness.Gen Hosp Psychiatry. 2020 Sep-Oct;66:96-102. doi: 10.1016/j.genhosppsych.2020.06.017. Epub 2020 Jul 2. Gen Hosp Psychiatry. 2020. PMID: 32763640 Free PMC article. Clinical Trial.
-
Characteristics of Mid-Term Post-Intensive Care Syndrome in Patients Attending a Follow-Up Clinic: A Prospective Comparison Between COVID-19 and Non-COVID-19 Survivors.Crit Care Explor. 2023 Jan 18;5(1):e0850. doi: 10.1097/CCE.0000000000000850. eCollection 2023 Jan. Crit Care Explor. 2023. PMID: 36699242 Free PMC article.
-
Virtualized clinical studies to assess the natural history and impact of gut microbiome modulation in non-hospitalized patients with mild to moderate COVID-19 a randomized, open-label, prospective study with a parallel group study evaluating the physiologic effects of KB109 on gut microbiota structure and function: a structured summary of a study protocol for a randomized controlled study.Trials. 2021 Apr 2;22(1):245. doi: 10.1186/s13063-021-05157-0. Trials. 2021. PMID: 33810796 Free PMC article.
-
Society of Critical Care Medicine's International Consensus Conference on Prediction and Identification of Long-Term Impairments After Critical Illness.Crit Care Med. 2020 Nov;48(11):1670-1679. doi: 10.1097/CCM.0000000000004586. Crit Care Med. 2020. PMID: 32947467 Review.
-
Six-Minute Walk Distance After Critical Illness: A Systematic Review and Meta-Analysis.J Intensive Care Med. 2021 Mar;36(3):343-351. doi: 10.1177/0885066619885838. Epub 2019 Nov 5. J Intensive Care Med. 2021. PMID: 31690160 Free PMC article.
Cited by
-
Exploring the effectiveness of eHealth interventions in treating Post Intensive Care Syndrome (PICS) outcomes: a systematic review.Crit Care. 2024 Sep 27;28(1):317. doi: 10.1186/s13054-024-05089-6. Crit Care. 2024. PMID: 39334262 Free PMC article.
-
Post-intensive care syndrome follow-up system after hospital discharge: a narrative review.J Intensive Care. 2024 Jan 12;12(1):2. doi: 10.1186/s40560-023-00716-w. J Intensive Care. 2024. PMID: 38217059 Free PMC article. Review.
References
-
- Iwashyna TJ, Cooke CR, Wunsch H, Kahn JM. Population burden of long-term survivorship after severe sepsis in older Americans. J Am Geriatr Soc. 2012 Jun 29;60(6):1070–7. doi: 10.1111/j.1532-5415.2012.03989.x. http://hdl.handle.net/2027.42/93626 - DOI - PMC - PubMed
-
- Griffiths J, Hatch RA, Bishop J, Morgan K, Jenkinson C, Cuthbertson BH, Brett SJ. An exploration of social and economic outcome and associated health-related quality of life after critical illness in general intensive care unit survivors: a 12-month follow-up study. Crit Care. 2013 May 28;17(3):R100. doi: 10.1186/cc12745. https://ccforum.biomedcentral.com/articles/10.1186/cc12745 cc12745 - DOI - DOI - PMC - PubMed
-
- Prescott HC, Langa KM, Iwashyna TJ. Readmission diagnoses after hospitalization for severe sepsis and other acute medical conditions. JAMA. 2015 Mar 10;313(10):1055–7. doi: 10.1001/jama.2015.1410. https://europepmc.org/abstract/MED/25756444 2190975 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
