

Treat-to-Target or High-Intensity Statin in Patients With Coronary Artery Disease: A Randomized Clinical Trial
- PMID: 36877807
- PMCID: PMC9989958
- DOI: 10.1001/jama.2023.2487
Treat-to-Target or High-Intensity Statin in Patients With Coronary Artery Disease: A Randomized Clinical Trial
Abstract
Importance: In patients with coronary artery disease, some guidelines recommend initial statin treatment with high-intensity statins to achieve at least a 50% reduction in low-density lipoprotein cholesterol (LDL-C). An alternative approach is to begin with moderate-intensity statins and titrate to a specific LDL-C goal. These alternatives have not been compared head-to-head in a clinical trial involving patients with known coronary artery disease.
Objective: To assess whether a treat-to-target strategy is noninferior to a strategy of high-intensity statins for long-term clinical outcomes in patients with coronary artery disease.
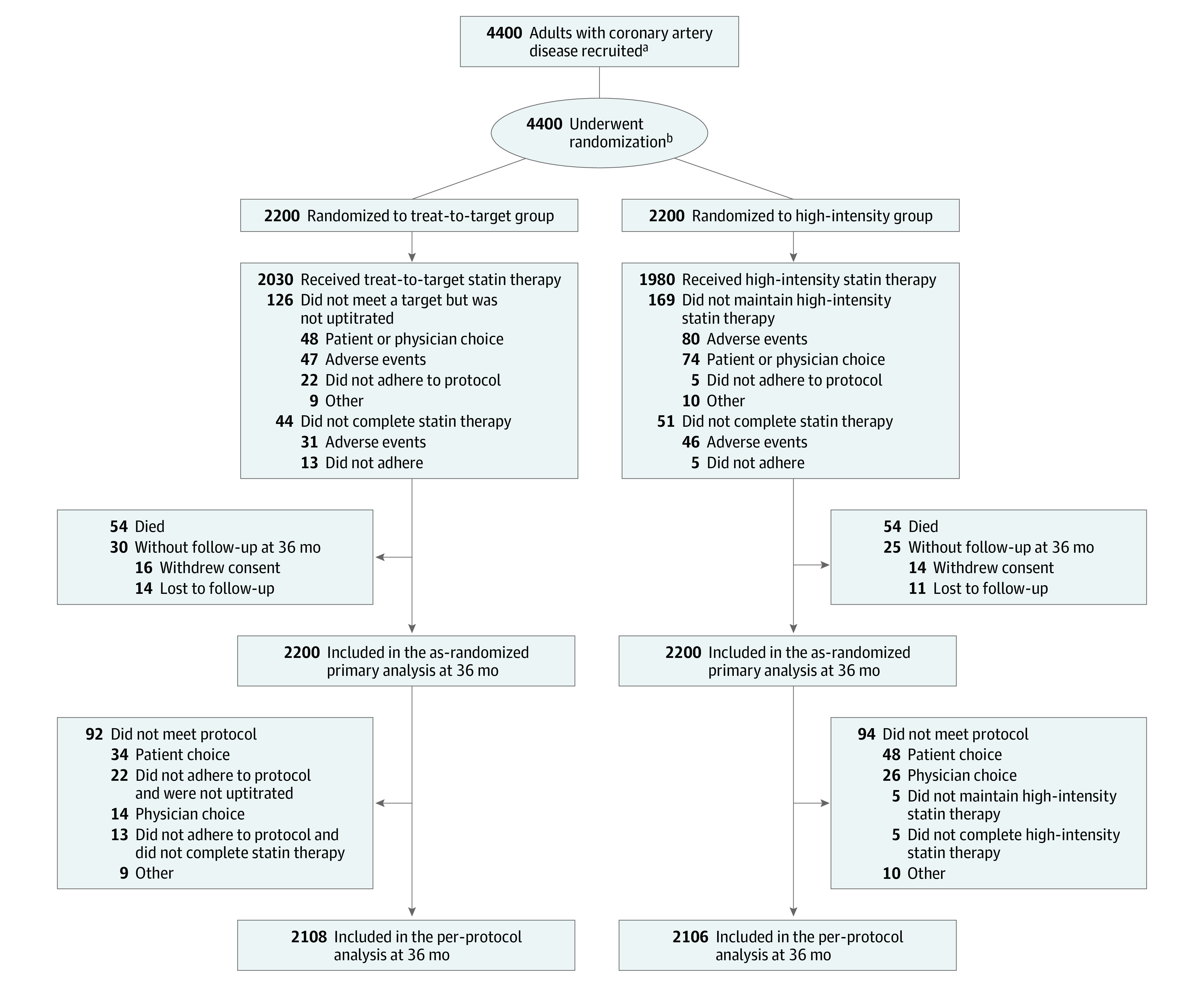
Design, setting, and participants: A randomized, multicenter, noninferiority trial in patients with a coronary disease diagnosis treated at 12 centers in South Korea (enrollment: September 9, 2016, through November 27, 2019; final follow-up: October 26, 2022).
Interventions: Patients were randomly assigned to receive either the LDL-C target strategy, with an LDL-C level between 50 and 70 mg/dL as the target, or high-intensity statin treatment, which consisted of rosuvastatin, 20 mg, or atorvastatin, 40 mg.
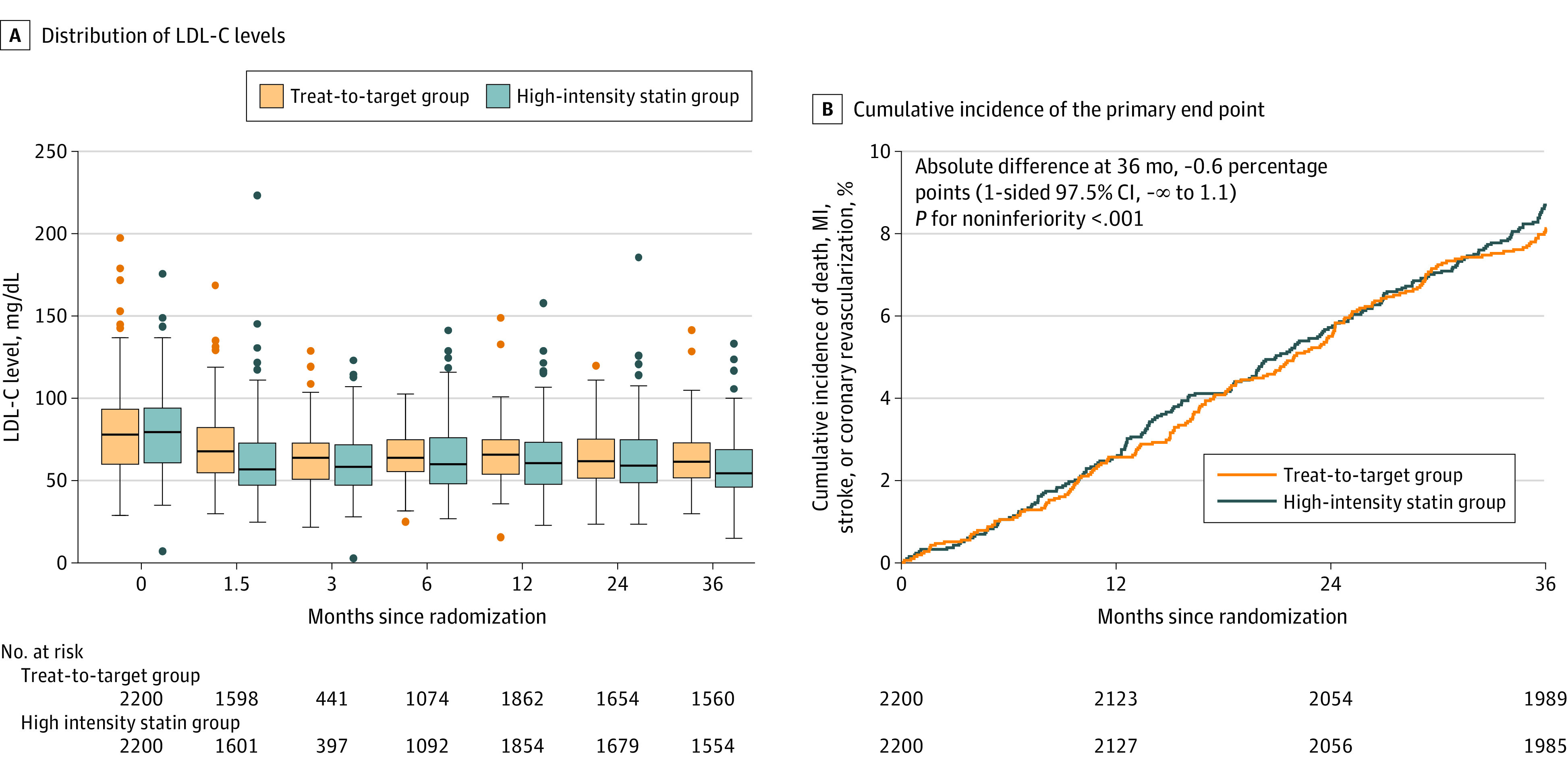
Main outcomes and measures: Primary end point was a 3-year composite of death, myocardial infarction, stroke, or coronary revascularization with a noninferiority margin of 3.0 percentage points.
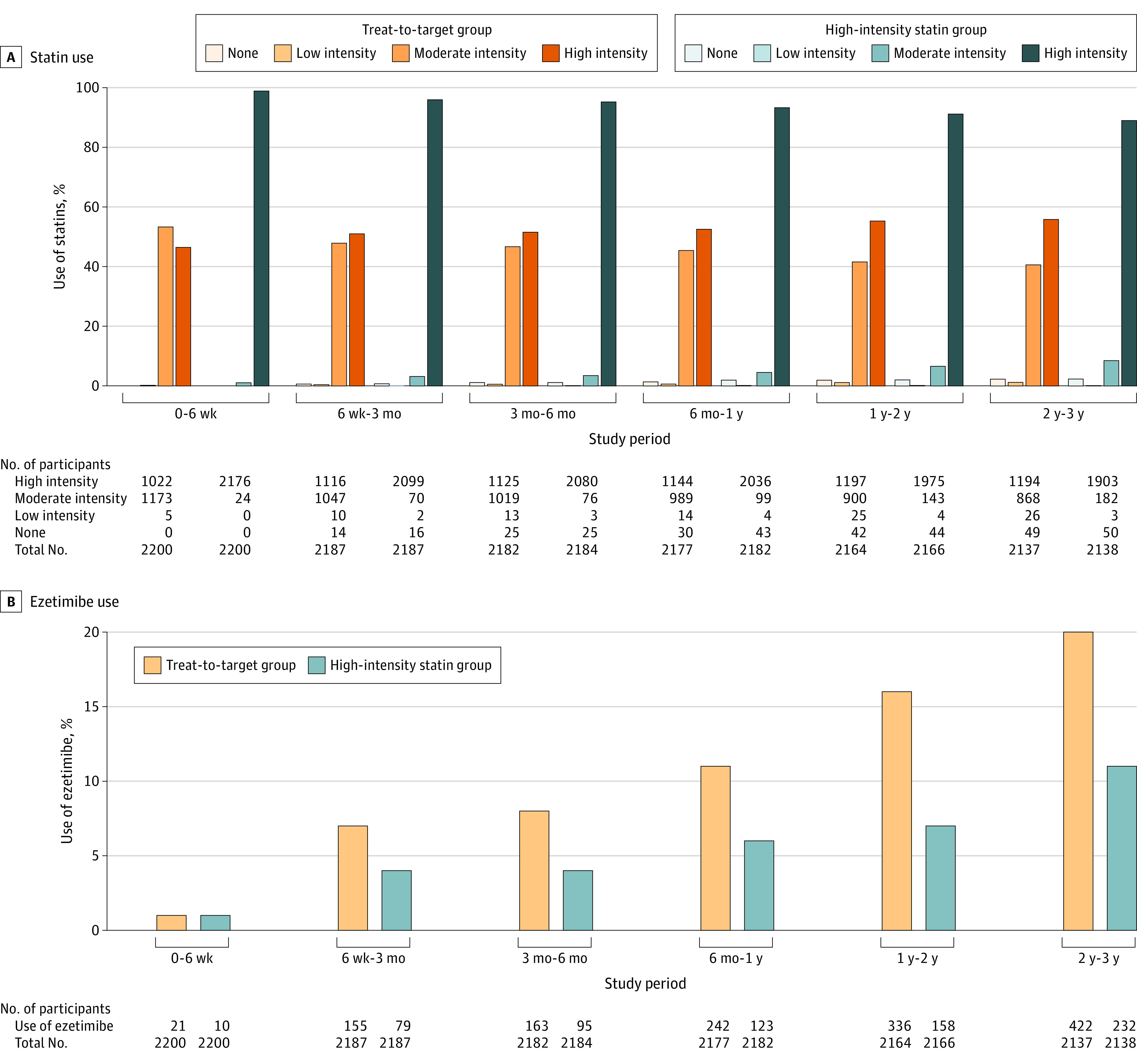
Results: Among 4400 patients, 4341 patients (98.7%) completed the trial (mean [SD] age, 65.1 [9.9] years; 1228 females [27.9%]). In the treat-to-target group (n = 2200), which had 6449 person-years of follow-up, moderate-intensity and high-intensity dosing were used in 43% and 54%, respectively. The mean (SD) LDL-C level for 3 years was 69.1 (17.8) mg/dL in the treat-to-target group and 68.4 (20.1) mg/dL in the high-intensity statin group (n = 2200) (P = .21, compared with the treat-to-target group). The primary end point occurred in 177 patients (8.1%) in the treat-to-target group and 190 patients (8.7%) in the high-intensity statin group (absolute difference, -0.6 percentage points [upper boundary of the 1-sided 97.5% CI, 1.1 percentage points]; P < .001 for noninferiority).
Conclusions and relevance: Among patients with coronary artery disease, a treat-to-target LDL-C strategy of 50 to 70 mg/dL as the goal was noninferior to a high-intensity statin therapy for the 3-year composite of death, myocardial infarction, stroke, or coronary revascularization. These findings provide additional evidence supporting the suitability of a treat-to-target strategy that may allow a tailored approach with consideration for individual variability in drug response to statin therapy.
Trial registration: ClinicalTrials.gov Identifier: NCT02579499.
Conflict of interest statement
Figures
Comment in
-
In CAD, treat-to-target statins were noninferior to high-intensity statins for a composite clinical outcome.Ann Intern Med. 2023 Jul;176(7):JC74. doi: 10.7326/J23-0041. Epub 2023 Jul 4. Ann Intern Med. 2023. PMID: 37399550
-
Treating Coronary Artery Disease With Treat-to-Target or High-Intensity Statin.JAMA. 2023 Aug 1;330(5):470-471. doi: 10.1001/jama.2023.9363. JAMA. 2023. PMID: 37526727 No abstract available.
References
-
- Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;139(25):e1082-e1143. - PMC - PubMed
-
- Baigent C, Blackwell L, Emberson J, et al. ; Cholesterol Treatment Trialists’ (CTT) Collaboration . Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376(9753):1670-1681. doi: 10.1016/S0140-6736(10)61350-5 - DOI - PMC - PubMed
-
- Stone NJ, Robinson JG, Lichtenstein AH, et al. ; American College of Cardiology/American Heart Association Task Force on Practice Guidelines . 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(25)(suppl 2):S1-S45. doi: 10.1161/01.cir.0000437738.63853.7a - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
