

Clinico-pathological features of diabetic and non-diabetic renal diseases in type 2 diabetic patients: a retrospective study from a 10-year experience in a single center
- PMID: 36879071
- PMCID: PMC10406681
- DOI: 10.1007/s11255-023-03478-4
Clinico-pathological features of diabetic and non-diabetic renal diseases in type 2 diabetic patients: a retrospective study from a 10-year experience in a single center
Abstract
Aim: To compare clinical and pathological characteristics as well as prognosis between diabetic nephropathy (DN) and non-diabetic renal disease (NDRD) so as to explore potential diagnostic criteria of DN and provide some guidance for the treatment of type 2 diabetes mellitus (T2DM) patients with kidney involvement.
Methods: T2DM patients with renal impairment who underwent kidney biopsy were included in this study, who were classified into 3 groups (DN, NDRD, DN with NDRD) based on their renal pathological diagnosis. Baseline clinical characteristics as well as follow-up data were collected and analyzed among 3 groups. Logistic regression was performed to determine the best predictors for DN diagnosis. Additional 34 MN patients without diabetes were enrolled by propensity score matching method to compare serum PLA2R antibody titer and kidney outcomes between diabetic MN patients and MN alone.
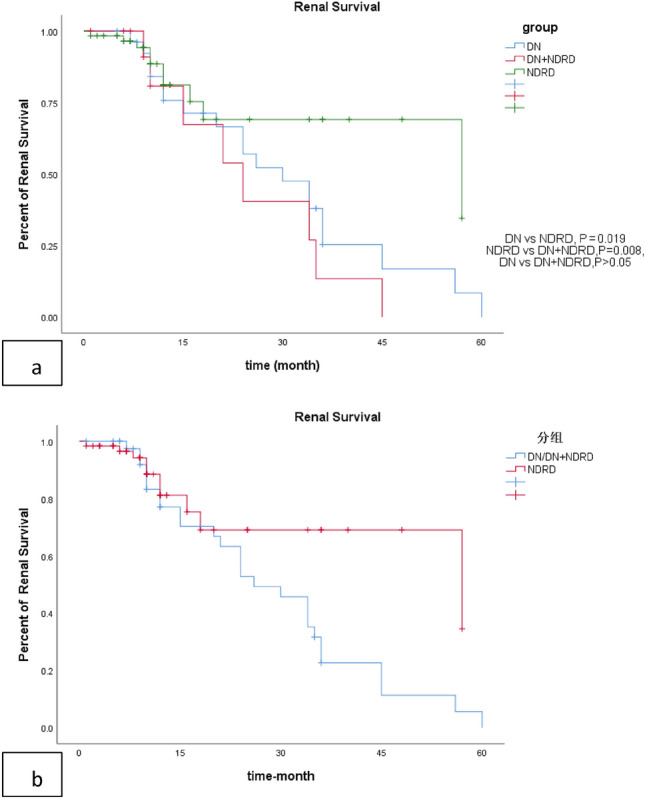
Results: Among 365 patients with type 2 diabetes who underwent kidney biopsy, 179 (49.0%) patients were diagnosed with NDRD alone and 37 (10.1%) patients with NDRD combined DN. Risk factors for DN development in T2DM patients were longer time since diabetes diagnosis, higher level of serum creatinine, absence of hematuria and presence of diabetic retinopathy by multivariate analysis. Lower rate of proteinuria remission and higher risk of renal progression were observed in DN group compared with NDRD group. Membranous nephropathy was the most common NDRD in diabetic patients. There was no difference in serum PLA2R antibody positiveness or titer between MN patients with or without T2DM. There was lower remission rate but similar renal progression in diabetic MN when age, gender, baseline eGFR, albuminuria and IFTA score were adjusted.
Conclusions: Non-diabetic renal disease is not uncommon in T2DM patients with renal impairment, which has better prognosis with proper treatment. Coexisting diabetic status does not exert negative impact on renal progression in MN patients, and immunosuppressive agents should be administered when necessary.
Keywords: Diabetic retinopathy; Membranous nephropathy; PLA2R antibody; Renal biopsy; Type 2 diabetes mellitus.
© 2023. The Author(s).
Conflict of interest statement
Authors declare no conflicts of interest.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
