

Vaccines as treatments for prostate cancer
- PMID: 36879114
- PMCID: PMC9987387
- DOI: 10.1038/s41585-023-00739-w
Vaccines as treatments for prostate cancer
Abstract
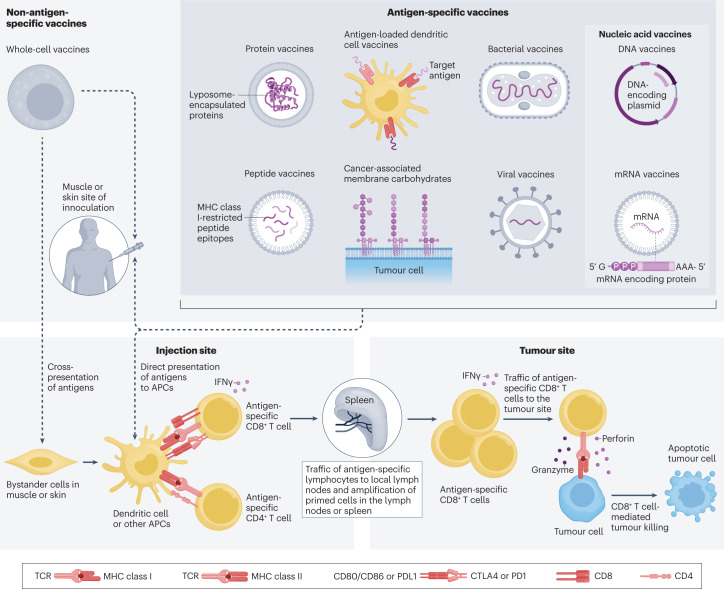
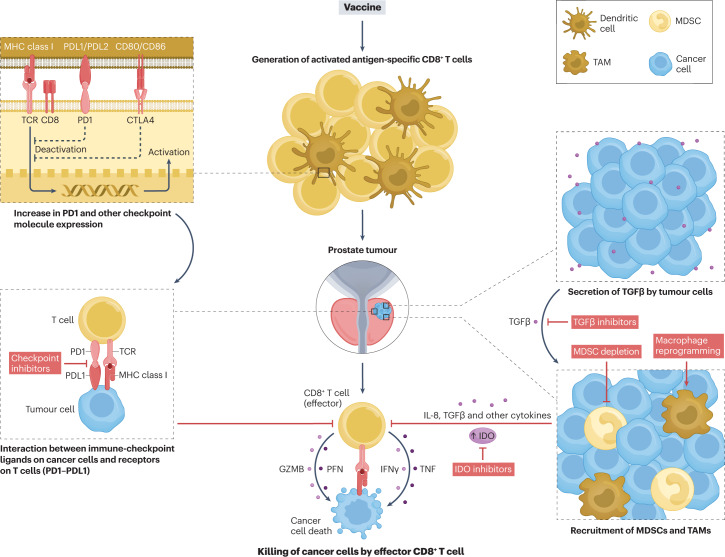
Prostate cancer is a leading cause of death in men worldwide. For over 30 years, growing interest has focused on the development of vaccines as treatments for prostate cancer, with the goal of using vaccines to activate immune cells capable of targeting prostate cancer to either eradicate recurrent disease or at least delay disease progression. This interest has been prompted by the prevalence and long natural history of the disease and by the fact that the prostate is an expendable organ. Thus, an immune response elicited by vaccination might not need to target the tumour uniquely but could theoretically target any prostate tissue. To date, different vaccine approaches and targets for prostate cancer have been evaluated in clinical trials. Overall, five approaches have been assessed in randomized phase III trials and sipuleucel-T was approved as a treatment for metastatic castration-resistant prostate cancer, being the only vaccine approved to date by the FDA as a treatment for cancer. Most vaccine approaches showed safety and some evidence of immunological activity but had poor clinical activity when used as monotherapies. However, increased activity has been observed when these vaccines were used in combination with other immune-modulating therapies. This evidence suggests that, in the future, prostate cancer vaccines might be used to activate and expand tumour-specific T cells as part of combination approaches with agents that target tumour-associated immune mechanisms of resistance.
© 2023. Springer Nature Limited.
Conflict of interest statement
D.G.M. has ownership interest, has received research support and serves as consultant to Madison Vaccines, Inc., which has licensed material described in this manuscript. The other authors declare no competing interests.
Figures
Similar articles
-
Sipuleucel-T: APC 8015, APC-8015, prostate cancer vaccine--Dendreon.Drugs R D. 2006;7(3):197-201. doi: 10.2165/00126839-200607030-00006. Drugs R D. 2006. PMID: 16752945 Review.
-
Advances in prostate cancer immunotherapies.Drugs Aging. 2007;24(3):197-221. doi: 10.2165/00002512-200724030-00003. Drugs Aging. 2007. PMID: 17362049 Review.
-
Current vaccination strategies for prostate cancer.Eur Urol. 2012 Feb;61(2):290-306. doi: 10.1016/j.eururo.2011.09.020. Epub 2011 Oct 3. Eur Urol. 2012. PMID: 22001436 Review.
-
Prime-boost vaccination targeting prostatic acid phosphatase (PAP) in patients with metastatic castration-resistant prostate cancer (mCRPC) using Sipuleucel-T and a DNA vaccine.J Immunother Cancer. 2018 Mar 13;6(1):21. doi: 10.1186/s40425-018-0333-y. J Immunother Cancer. 2018. PMID: 29534736 Free PMC article. Clinical Trial.
-
Prostate cancer vaccines: current status and future potential.BioDrugs. 2008;22(2):71-84. doi: 10.2165/00063030-200822020-00001. BioDrugs. 2008. PMID: 18345705 Review.
Cited by
-
Nanomaterials augmented bioeffects of ultrasound in cancer immunotherapy.Mater Today Bio. 2023 Dec 22;24:100926. doi: 10.1016/j.mtbio.2023.100926. eCollection 2024 Feb. Mater Today Bio. 2023. PMID: 38179429 Free PMC article. Review.
-
Translational Advances in Oncogene and Tumor-Suppressor Gene Research.Cancers (Basel). 2025 Mar 17;17(6):1008. doi: 10.3390/cancers17061008. Cancers (Basel). 2025. PMID: 40149342 Free PMC article. Review.
-
PD-1 blockade employed at the time CD8+ T cells are activated enhances their antitumor efficacy.J Immunother Cancer. 2025 May 7;13(5):e011145. doi: 10.1136/jitc-2024-011145. J Immunother Cancer. 2025. PMID: 40341032 Free PMC article.
-
Immunotherapy Vaccines for Prostate Cancer Treatment.Cancer Med. 2024 Oct;13(20):e70294. doi: 10.1002/cam4.70294. Cancer Med. 2024. PMID: 39463159 Free PMC article. Review.
-
Development and Optimal Immune Strategy of an Alum-Stabilized Pickering emulsion for Cancer Vaccines.Vaccines (Basel). 2023 Jun 28;11(7):1169. doi: 10.3390/vaccines11071169. Vaccines (Basel). 2023. PMID: 37514985 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
