

Effects of music therapy as an alternative treatment on depression in children and adolescents with ADHD by activating serotonin and improving stress coping ability
- PMID: 36879223
- PMCID: PMC9987133
- DOI: 10.1186/s12906-022-03832-6
Effects of music therapy as an alternative treatment on depression in children and adolescents with ADHD by activating serotonin and improving stress coping ability
Abstract
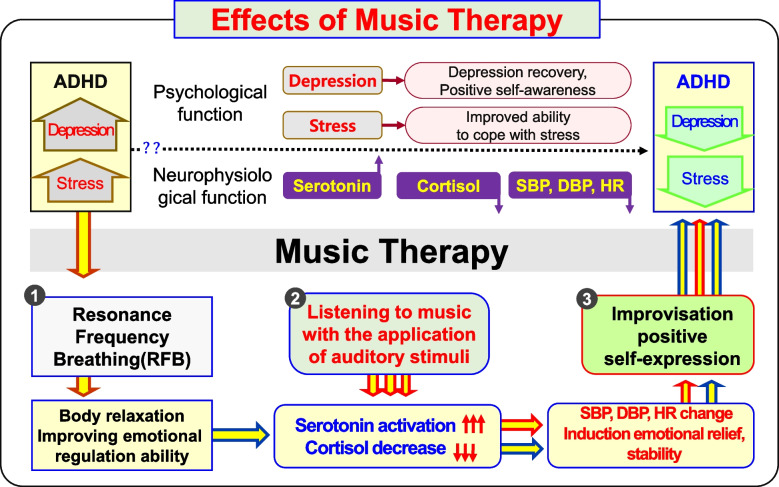
Objective: The objective of this study was to determine the effect of music therapy as an alternative treatment on depression in children and adolescents with attention-deficit hyperactivity disorder (ADHD) by activating serotonin (5-HT) and improving stress coping ability.
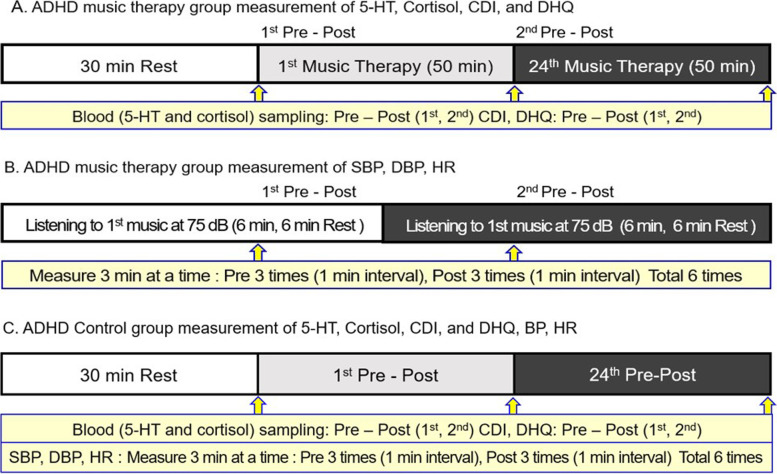
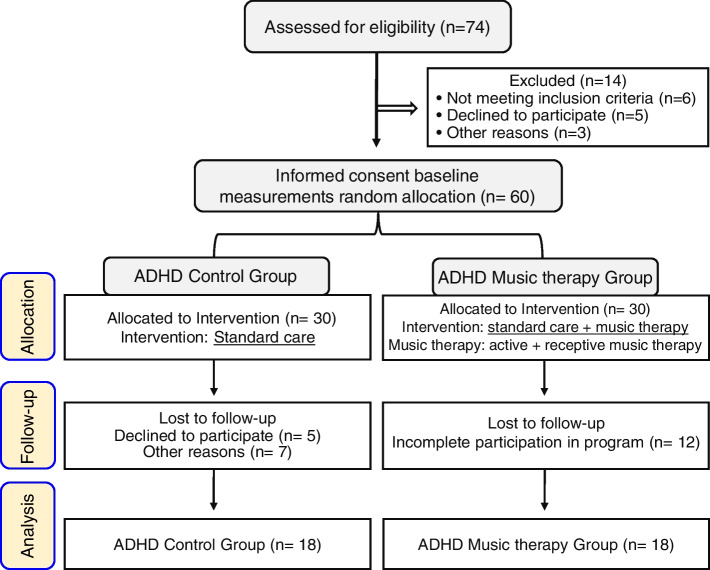
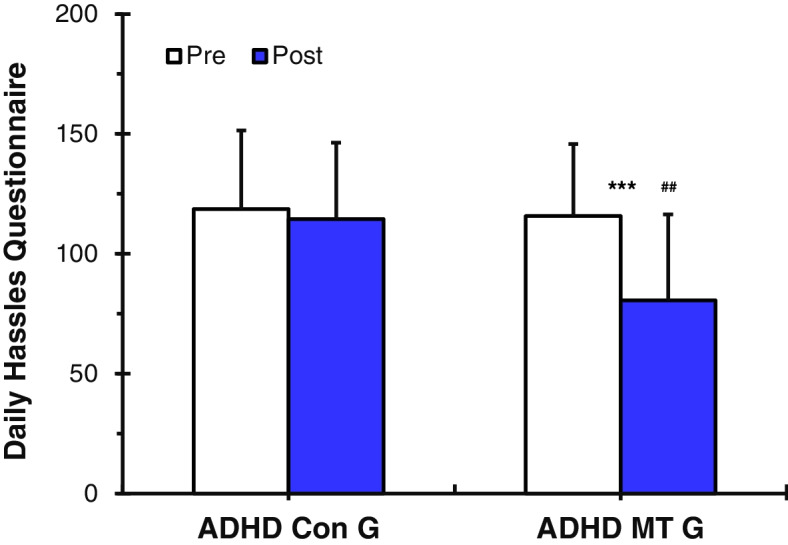
Methods: This study is designed based on randomization method. A total of 36 subjects participated in the experiment, consisting of an ADHD control group (n = 18) and ADHD music therapy group (n = 18). The ADHD control group received standard care, while the ADHD music therapy group received music therapy and standard care. The ADHD music therapy group received both active music therapy (improvisation) and receptive music therapy (music listening) for 50 minutes, twice a week, for 3 months: a total of 24 times. From a neurophysiological perspective, changes in depression and stress were tracked by measuring 5-HT secretion, cortisol expression, blood pressure (BP), heart rate (HR), and CDI and DHQ psychological scales.
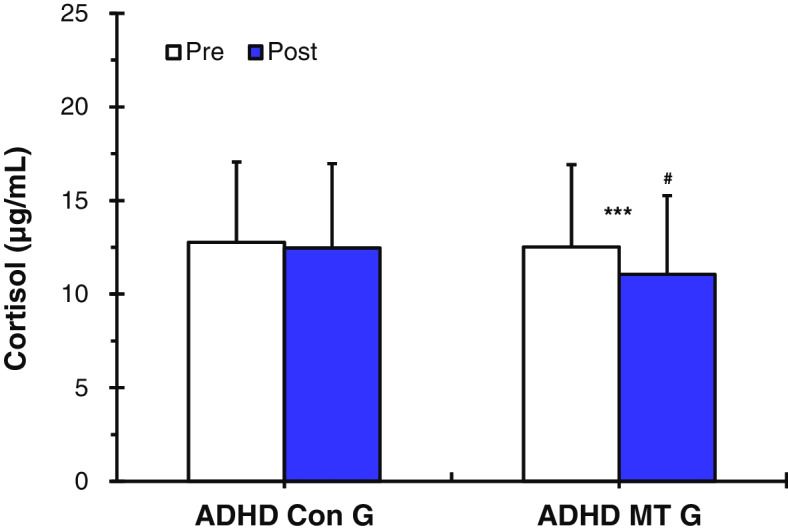
Results: The ADHD music therapy group's 5-HT secretion increased (p < 0.001), whereas cortisol expression (p < 0.001), BP (p < 0.001) and HR (p < 0.001) decreased. The CDI and DHQ psychological scales also showed positive changes (p < 0.01 and p < 0.001, respectively). However, the ADHD Con G's (who did not receive music therapy) 5-HT secretion did not increase, whereas cortisol expression, BP, and HR did not decrease. In addition, the CDI and DHQ psychological scales did not display positive changes.
Conclusions: In conclusion, the application of music therapy as an alternative treatment for ADHD children and adolescents showed positive neurophysiological and psychological effects. Therefore, this study would like to propose a new alternative to medicine for preventing and treating depression through various uses of music therapy.
Keywords: Ability to address stress; BP; Children and adolescents with ADHD; Cortisol; Depression; HR; Music therapy; Serotonin (5-HT).
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
