

Science fiction or clinical reality: a review of the applications of artificial intelligence along the continuum of trauma care
- PMID: 36879293
- PMCID: PMC9987401
- DOI: 10.1186/s13017-022-00469-1
Science fiction or clinical reality: a review of the applications of artificial intelligence along the continuum of trauma care
Abstract
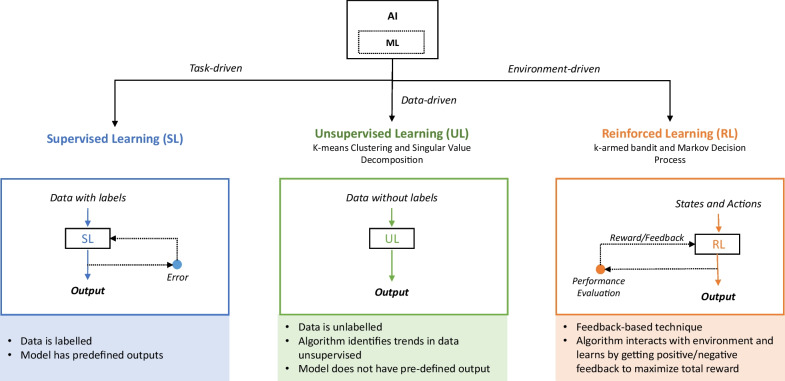
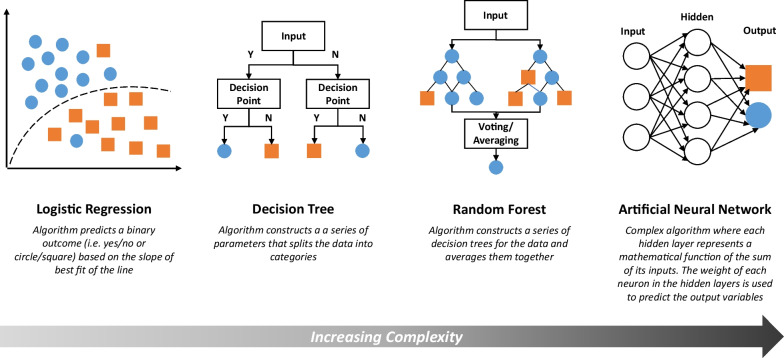
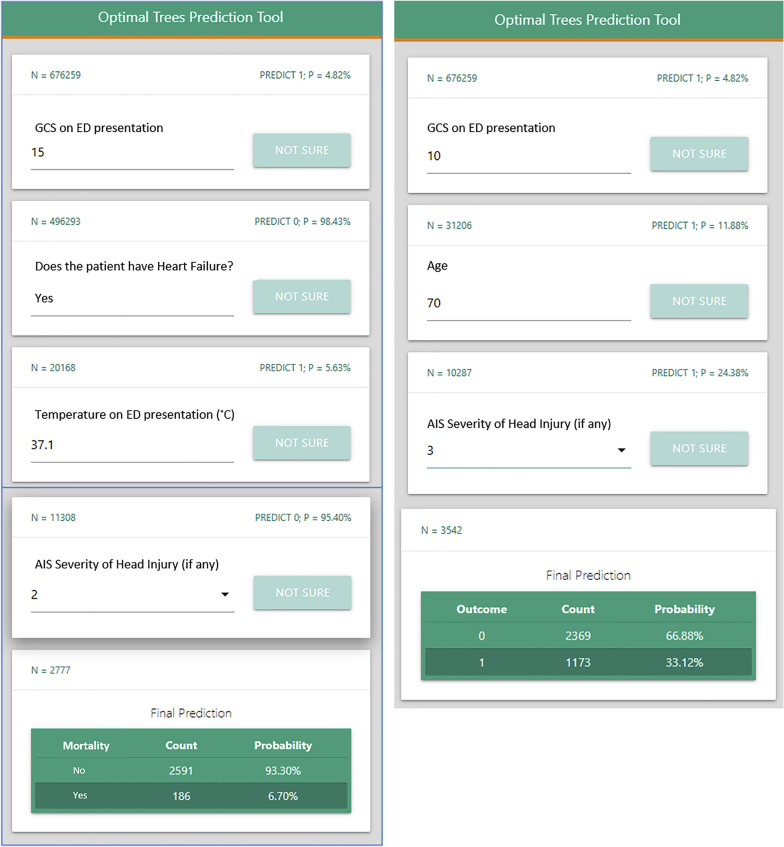
Artificial intelligence (AI) and machine learning describe a broad range of algorithm types that can be trained based on datasets to make predictions. The increasing sophistication of AI has created new opportunities to apply these algorithms within within trauma care. Our paper overviews the current uses of AI along the continuum of trauma care, including injury prediction, triage, emergency department volume, assessment, and outcomes. Starting at the point of injury, algorithms are being used to predict severity of motor vehicle crashes, which can help inform emergency responses. Once on the scene, AI can be used to help emergency services triage patients remotely in order to inform transfer location and urgency. For the receiving hospital, these tools can be used to predict trauma volumes in the emergency department to help allocate appropriate staffing. After patient arrival to hospital, these algorithms not only can help to predict injury severity, which can inform decision-making, but also predict patient outcomes to help trauma teams anticipate patient trajectory. Overall, these tools have the capability to transform trauma care. AI is still nascent within the trauma surgery sphere, but this body of the literature shows that this technology has vast potential. AI-based predictive tools in trauma need to be explored further through prospective trials and clinical validation of algorithms.
Keywords: Artificial intelligence; Machine learning; Trauma.
© 2023. The Author(s).
Conflict of interest statement
Dr. Hameed and Mr. Bandurski are founders of T6 Health Systems, a health information technology company focusing on data collection and analysis during trauma resuscitation. The other authors declare that they have no competing interests.
Figures
References
-
- Morales EF, Escalante HJ. Chapter 6—a brief introduction to supervised, unsupervised, and reinforcement learning. In: Torres-García AA, Reyes-García CA, Villaseñor-Pineda L, Mendoza-Montoya O, editors. Biosignal processing and classification using computational learning and intelligence. Academic Press; 2022. pp. 111–129.
-
- Singh A, Thakur N, Sharma A (eds). A review of supervised machine learning algorithms. In: 2016 3rd international conference on computing for sustainable global development (INDIACom); 2016. p. 1310–5.
-
- Zou J, Han Y, So S-S. Overview of artificial neural networks. In: Livingstone DJ, editor. Artificial neural networks: methods and applications. Totowa: Humana Press; 2009. pp. 14–22.
