

Nomogram for predicting the risk of postoperative myasthenic crisis in patients with thymectomy
- PMID: 36879415
- PMCID: PMC10109272
- DOI: 10.1002/acn3.51752
Nomogram for predicting the risk of postoperative myasthenic crisis in patients with thymectomy
Abstract
Objective: This study aimed to develop and validate internally a clinical predictive model, for predicting myasthenic crisis within 30 days after thymectomy in patients with myasthenia gravis.
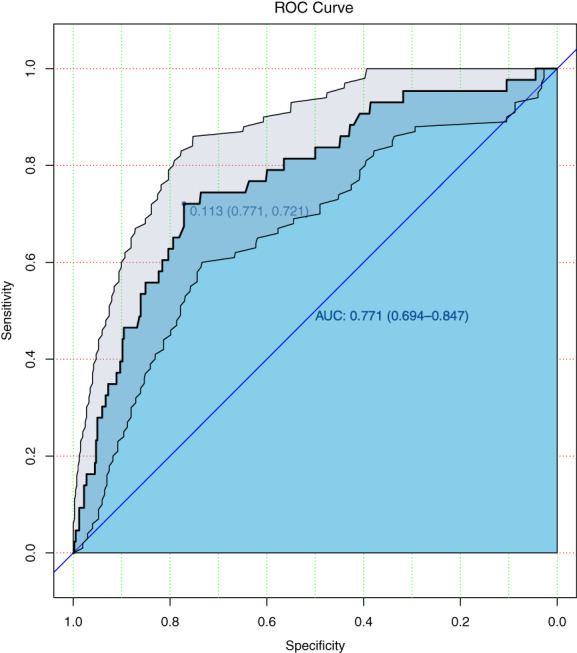
Methods: Eligible patients were enrolled between January 2015 and May 2019. The primary outcome measure was postoperative myasthenic crisis (POMC). A predictive model was constructed using logistic regression and presented in a nomogram. The area under the receiver operating characteristic curve (AUC) was calculated to examine the performance. The study population was divided into high- and low-risk groups according to Youden index. Calibration curves with 1000 replications bootstrap resampling were plotted to visualize the calibration of the nomogram. Decision curve analyses (DCA) with 1000 replications bootstrap resampling were performed to evaluate the clinical usefulness of the model.
Results: A total of 445 patients were enrolled. Five variables were screened including thymus imaging, onset age, MGFA classification, preoperative treatment regimen, and surgical approach. The model exhibited moderate discriminative ability with AUC value 0.771. The threshold probability was 0.113, which was used to differentiate between high- and low-risk groups. The sensitivity and specificity were 72.1% and 77.1%, respectively. The high-risk group had an 8.70-fold higher risk of POMC. The calibration plot showed that when the probability was between 0 and 0.5, the deviation calibration curve of the model was consistent with the ideal curve.
Interpretation: This nomogram could assist in identifying patients at higher risk of POMC and determining the optimal surgical time for these patients.
© 2023 The Authors. Annals of Clinical and Translational Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous