

Effectivity of the Outside-In Pie-Crusting Technique and an All-Inside Meniscal Repair Device in the Repair of Ramp Lesions
- PMID: 36879867
- PMCID: PMC9984773
- DOI: 10.1016/j.eats.2022.11.002
Effectivity of the Outside-In Pie-Crusting Technique and an All-Inside Meniscal Repair Device in the Repair of Ramp Lesions
Abstract
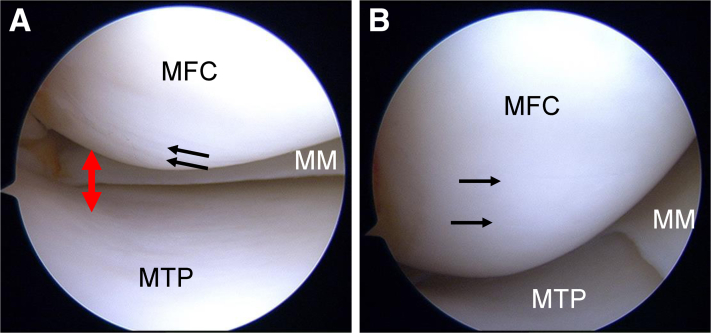
Ramp lesions are characteristic medial meniscus injuries seen in anterior cruciate ligament-injured knees. Anterior cruciate ligament injuries combined with ramp lesions increase the amount of anterior tibial translation and tibial external rotation. Therefore, the diagnosis and treatment of ramp lesions have received increasing attention. However, ramp lesions can be difficult to diagnose on preoperative magnetic resonance imaging. Additionally, ramp lesions are difficult to observe and treat intraoperatively in the posteromedial compartment. Although good results have been reported with the use of a suture hook through the posteromedial portal in the treatment of ramp lesions, the complexity and difficulty of the technique are further problems. The outside-in pie-crusting technique is a simple procedure that can enlarge the medial compartment and facilitate the observation and repair of ramp lesions. After this technique, ramp lesions can be properly sutured, using an all-inside meniscal repair device, without damaging the surrounding cartilage. A combination of the outside-in pie-crusting technique and an all-inside meniscal repair device (with only anterior portals) is effective in the repair of ramp lesions. This Technical Note aims to report in detail the flow of a series of techniques, including our diagnostic and therapeutic methods.
© 2022 The Authors.
Figures










References
-
- Stephen J.M., Halewood C., Kittl C., Bollen S.R., Williams A., Amis A.A. Posteromedial meniscocapsular lesions increase tibiofemoral joint laxity with anterior cruciate ligament deficiency, and their repair reduces laxity. Am J Sports Med. 2016;44:400–408. - PubMed
-
- Malatray M., Raux S., Peltier A., Pfirrmann C., Seil R., Chotel F. Ramp lesions in ACL deficient knees in children and adolescent population: A high prevalence confirmed in intercondylar and posteromedial exploration. Knee Surg Sports Traumatol Arthrosc. 2018;26:1074–1079. - PubMed
-
- Kim S.H., Park Y.B., Won Y.S. An increased lateral femoral condyle ratio is an important risk factor for a medial meniscus ramp lesion including red-red zone tear. Arthroscopy. 2021;37:3159–3165. - PubMed
LinkOut - more resources
Full Text Sources
