

Modelling the impact of CD4 testing on mortality from TB and cryptococcal meningitis among patients with advanced HIV disease in nine countries
- PMID: 36880429
- PMCID: PMC9989935
- DOI: 10.1002/jia2.26070
Modelling the impact of CD4 testing on mortality from TB and cryptococcal meningitis among patients with advanced HIV disease in nine countries
Abstract
Introduction: Despite antiretroviral therapy (ART) scale-up among people living with HIV (PLHIV), those with advanced HIV disease (AHD) (defined in adults as CD4 count <200 cells/mm3 or clinical stage 3 or 4), remain at high risk of death from opportunistic infections. The shift from routine baseline CD4 testing towards viral load testing in conjunction with "Test and Treat" has limited AHD identification.
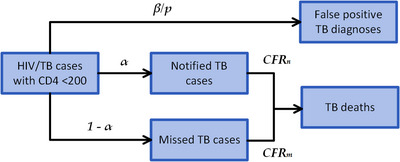
Methods: We used official estimates and existing epidemiological data to project deaths from tuberculosis (TB) and cryptococcal meningitis (CM) among PLHIV-initiating ART with CD4 <200 cells/mm3 , in the absence of select World Health Organization recommended diagnostic or therapeutic protocols for patients with AHD. We modelled the reduction in deaths, based on the performance of screening/diagnostic testing and the coverage and efficacy of treatment/preventive therapies for TB and CM. We compared projected TB and CM deaths in the first year of ART from 2019 to 2024, with and without CD4 testing. The analysis was performed for nine countries: South Africa, Kenya, Lesotho, Mozambique, Nigeria, Uganda, Zambia, Zimbabwe and the Democratic Republic of Congo.
Results: The effect of CD4 testing comes through increased identification of AHD and consequent eligibility for protocols for AHD prevention, diagnosis and management; algorithms for CD4 testing avert between 31% and 38% of deaths from TB and CM in the first year of ART. The number of CD4 tests required per death averted varies widely by country from approximately 101 for South Africa to 917 for Kenya.
Conclusions: This analysis supports retaining baseline CD4 testing to avert deaths from TB and CM, the two most deadly opportunistic infections among patients with AHD. However, national programmes will need to weigh the cost of increasing CD4 access against other HIV-related priorities and allocate resources accordingly.
Keywords: CD4 testing; TB mortality; advanced HIV disease; cryptococcal meningitis; deaths averted; mortality.
© 2023 The Authors. Journal of the International AIDS Society published by John Wiley & Sons Ltd on behalf of the International AIDS Society.
Conflict of interest statement
The authors have no competing interests.
Figures



References
-
- UNAIDS . Global HIV & AIDS statistics — 2021 fact sheet. 2021.
-
- WHO . Managing advanced HIV disease and rapid initiation of antiretrovial therapy. 2017. - PubMed
-
- WHO . Global tuberculosis report. 2018.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
