

Current patterns of trauma center proliferation have not led to proportionate improvements in access to care or mortality after injury: An ecologic study
- PMID: 36880704
- PMCID: PMC10208642
- DOI: 10.1097/TA.0000000000003940
Current patterns of trauma center proliferation have not led to proportionate improvements in access to care or mortality after injury: An ecologic study
Abstract
Background: Timely access to high-level (I/II) trauma centers (HLTCs) is essential to minimize mortality after injury. Over the last 15 years, there has been a proliferation of HLTC nationally. The current study evaluates the impact of additional HLTC on population access and injury mortality.
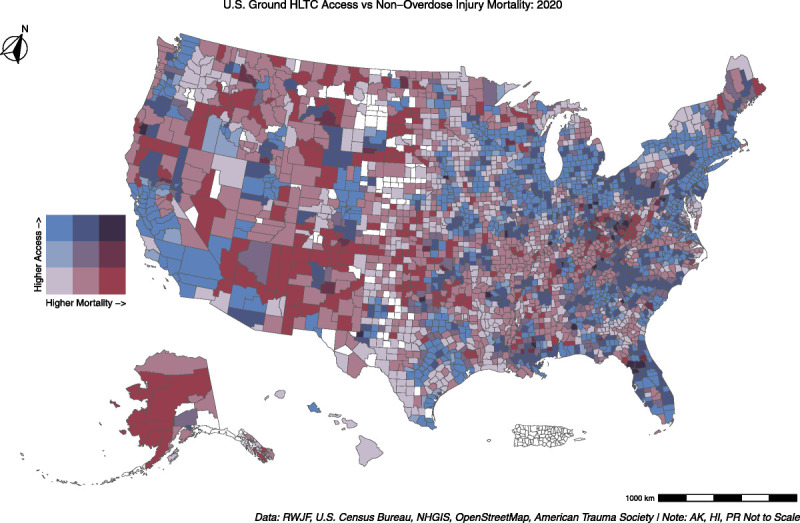
Methods: A geocoded list of HLTC, with year designated, was obtained from the American Trauma Society, and 60-minute travel time polygons were created using OpenStreetMap data. Census block group population centroids, county population centroids, and American Communities Survey data from 2005 and 2020 were integrated. Age-adjusted nonoverdose injury mortality was obtained from CDC Wide-ranging Online Data for Epidemiologic Research and the Robert Wood Johnson Foundation. Geographically weighted regression models were used to identify independent predictors of HLTC access and injury mortality.
Results: Over the 15-year (2005-2020) study period, the number of HLTC increased by 31.0% (445 to 583), while population access to HLTC increased by 6.9% (77.5-84.4%). Despite this increase, access was unchanged in 83.1% of counties, with a median change in access of 0.0% (interquartile range, 0.0-1.1%). Population-level age-adjusted injury mortality rates increased by 5.39 per 100,000 population during this time (60.72 to 66.11 per 100,000). Geographically weighted regression controlling for population demography and health indicators found higher median income and higher population density to be positively associated with majority (≥50%) HLTC population coverage and negatively associated with county-level nonoverdose mortality.
Conclusion: Over the past 15 years, the number of HLTC increased 31%, while population access to HLTC increased only 6.9%. High-level (I/II) trauma center designation is likely driven by factors other than population need. To optimize efficiency and decrease potential oversupply, the designation process should include population level metrics. Geographic information system methodology can be an effective tool to assess optimal placement.
Level of evidence: Prognostic and Epidemiological; Level IV.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Association for the Surgery of Trauma.
Figures


Similar articles
-
[Volume and health outcomes: evidence from systematic reviews and from evaluation of Italian hospital data].Epidemiol Prev. 2013 Mar-Jun;37(2-3 Suppl 2):1-100. Epidemiol Prev. 2013. PMID: 23851286 Italian.
-
Organised trauma systems and designated trauma centres for improving outcomes in injured patients.Cochrane Database Syst Rev. 2025 Aug 1;8(8):CD012500. doi: 10.1002/14651858.CD012500.pub2. Cochrane Database Syst Rev. 2025. PMID: 40747779 Free PMC article. Review.
-
Are new pediatric trauma centers located close to the high-risk populations? A geolocation study.J Trauma Acute Care Surg. 2024 Dec 1;97(6):943-947. doi: 10.1097/TA.0000000000004452. Epub 2024 Oct 1. J Trauma Acute Care Surg. 2024. PMID: 39350317
-
The Black Book of Psychotropic Dosing and Monitoring.Psychopharmacol Bull. 2024 Jul 8;54(3):8-59. Psychopharmacol Bull. 2024. PMID: 38993656 Free PMC article. Review.
-
Surveillance for Violent Deaths - National Violent Death Reporting System, 48 States, the District of Columbia, and Puerto Rico, 2020.MMWR Surveill Summ. 2023 May 26;72(5):1-38. doi: 10.15585/mmwr.ss7205a1. MMWR Surveill Summ. 2023. PMID: 37220104 Free PMC article.
Cited by
-
A Systematic Literature Review of Trauma Systems: An Operations Management Perspective.Adv Rehabil Sci Pract. 2025 Jan 16;14:27536351241310645. doi: 10.1177/27536351241310645. eCollection 2025 Jan-Dec. Adv Rehabil Sci Pract. 2025. PMID: 39830526 Free PMC article. Review.
-
Pediatric Readiness and Trauma Center Access for Children.JAMA Pediatr. 2025 Apr 1;179(4):455-462. doi: 10.1001/jamapediatrics.2024.6058. JAMA Pediatr. 2025. PMID: 39899287
-
Evaluation and Implication of Case Volume Variation in Level 1 and 2 Trauma Centers.Ann Surg Open. 2025 Jun 12;6(2):e589. doi: 10.1097/AS9.0000000000000589. eCollection 2025 Jun. Ann Surg Open. 2025. PMID: 40557357 Free PMC article.
-
Changes in payer mix of new and established trauma centers: the new trauma center money grab?Trauma Surg Acute Care Open. 2024 Jul 15;9(1):e001417. doi: 10.1136/tsaco-2024-001417. eCollection 2024. Trauma Surg Acute Care Open. 2024. PMID: 39161373 Free PMC article.
References
-
- Sampalis JS Lavoie A Boukas S Tamim H Nikolis A Frechette P, et al. . Trauma center designation: initial impact on trauma-related mortality. J Trauma. 1995;39(2):232–237. - PubMed
-
- MacKenzie EJ Rivara FP Jurkovich GJ Nathens AB Frey KP Egleston BL, et al. . A national evaluation of the effect of trauma-center care on mortality. N Engl J Med. 2006;354(4):366–378. - PubMed
-
- American College of Surgeons . Verification, Review, and Consultation Program. ACS. 2022. Available at: https://www.facs.org/quality-programs/trauma/quality/verification-review.... Accessed July 30, 2022.
-
- Mullins RJ Veum-Stone J Hedges JR Zimmer-Gembeck MJ Mann NC Southard PA, et al. . Influence of a statewide trauma system on location of hospitalization and outcome of injured patients. J Trauma. 1996;40(4):536–545; discussion 545-6. - PubMed
-
- Nathens AB, Jurkovich GJ, Cummings P, Rivara FP, Maier RV. The effect of organized systems of trauma care on motor vehicle crash mortality. JAMA. 2000;283(15):1990–1994. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
