

Effect of Induction Therapy With Olamkicept vs Placebo on Clinical Response in Patients With Active Ulcerative Colitis: A Randomized Clinical Trial
- PMID: 36881032
- PMCID: PMC9993185
- DOI: 10.1001/jama.2023.1084
Effect of Induction Therapy With Olamkicept vs Placebo on Clinical Response in Patients With Active Ulcerative Colitis: A Randomized Clinical Trial
Abstract
Importance: Olamkicept, a soluble gp130-Fc-fusion-protein, selectively inhibits interleukin 6 (IL-6) trans-signaling by binding the soluble IL-6 receptor/IL-6 complex. It has anti-inflammatory activities in inflammatory murine models without immune suppression.
Objective: To assess the effect of olamkicept as induction therapy in patients with active ulcerative colitis.
Design, setting, and participants: Randomized, double-blind, placebo-controlled phase 2 trial of olamkicept in 91 adults with active ulcerative colitis (full Mayo score ≥5, rectal bleeding score ≥1, endoscopy score ≥2) and an inadequate response to conventional therapy. The study was conducted at 22 clinical study sites in East Asia. Patients were recruited beginning in February 2018. Final follow-up occurred in December 2020.
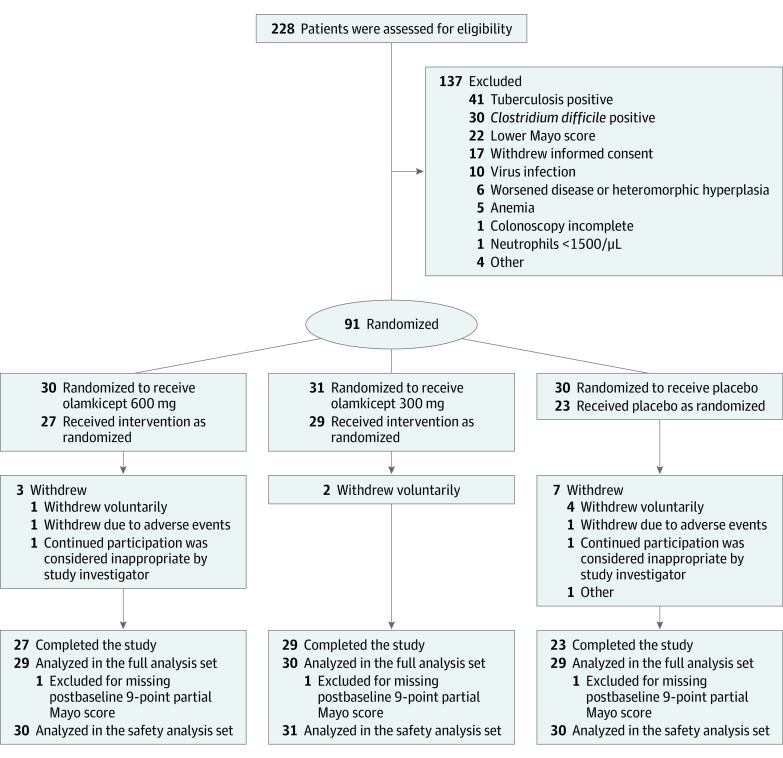
Interventions: Eligible patients were randomized 1:1:1 to receive a biweekly intravenous infusion of olamkicept 600 mg (n = 30) or 300 mg (n = 31) or placebo (n = 30) for 12 weeks.
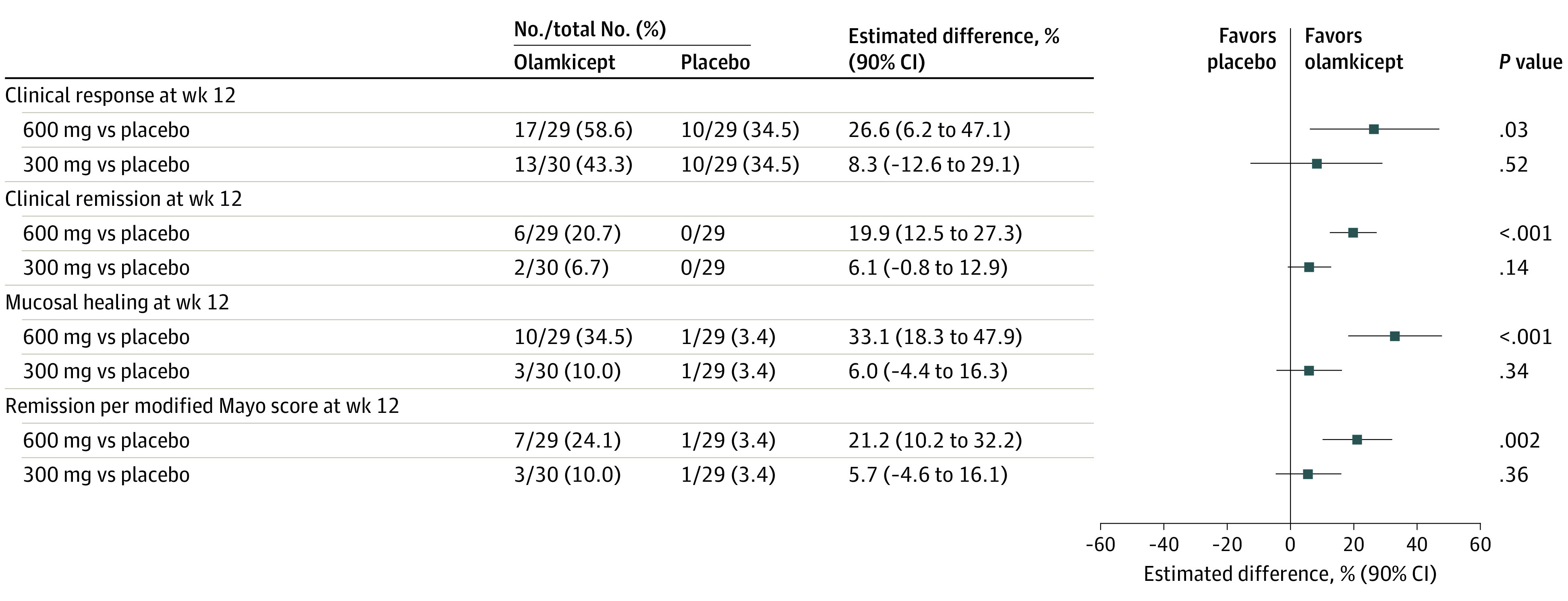
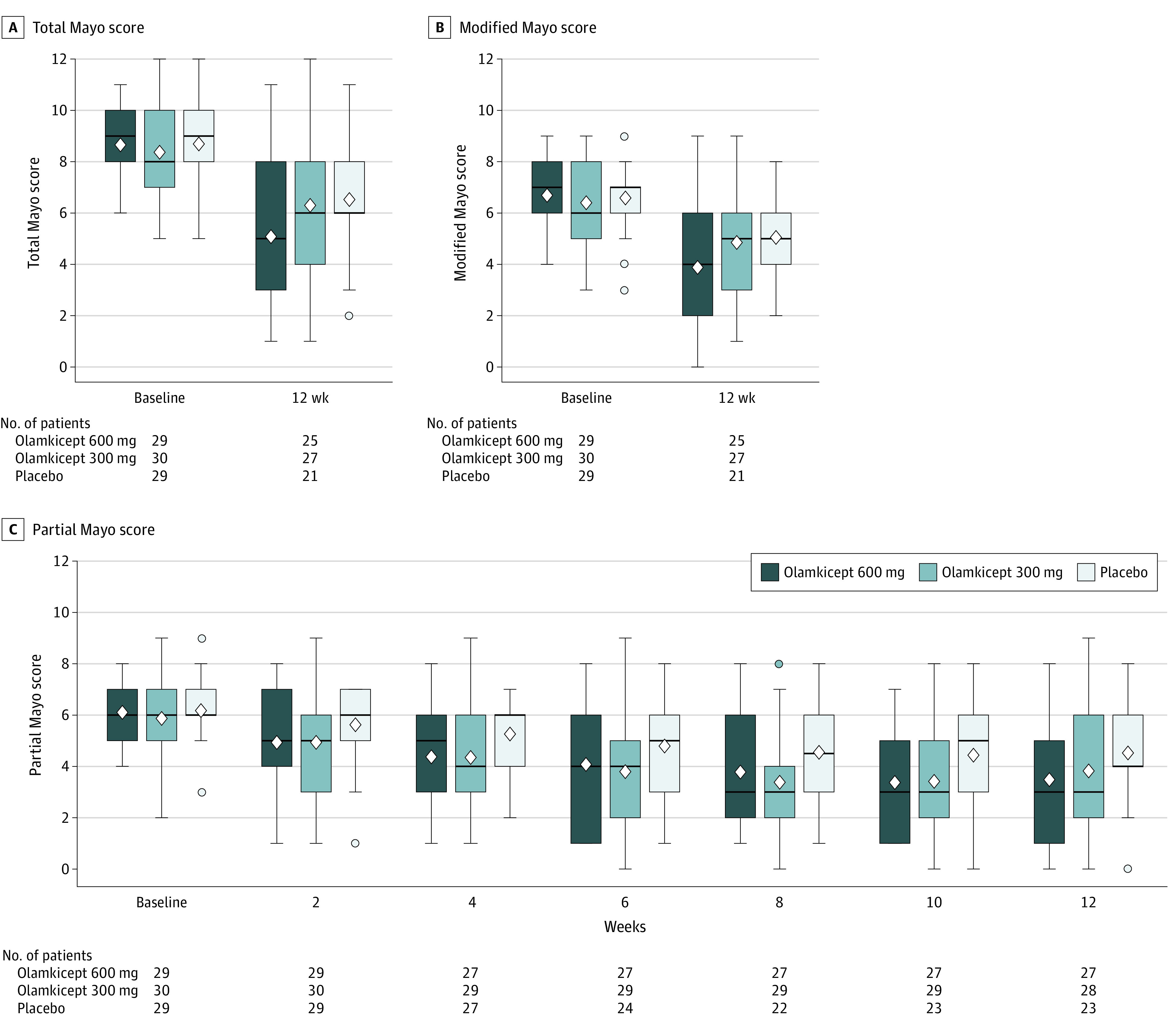
Main outcomes and measures: The primary end point was clinical response at week 12 (defined as ≥3 and ≥30% decrease from baseline total Mayo score; range, 0-12 [worst] with ≥1 decrease and ≤1 in rectal bleeding [range, 0-3 {worst}]). There were 25 secondary efficacy outcomes, including clinical remission and mucosal healing at week 12.
Results: Ninety-one patients (mean age, 41 years; 25 women [27.5%]) were randomized; 79 (86.8%) completed the trial. At week 12, more patients receiving olamkicept 600 mg (17/29 [58.6%]) or 300 mg (13/30 [43.3%]) achieved clinical response than placebo (10/29 [34.5%]), with adjusted difference vs placebo of 26.6% (90% CI, 6.2% to 47.1%; P = .03) for 600 mg and 8.3% (90% CI, -12.6% to 29.1%; P = .52) for 300 mg. Among patients randomized to receive 600 mg olamkicept, 16 of 25 secondary outcomes were statistically significant compared with placebo. Among patients randomized to receive 300 mg, 6 of 25 secondary outcomes were statistically significant compared with placebo. Treatment-related adverse events occurred in 53.3% (16/30) of patients receiving 600 mg olamkicept, 58.1% (18/31) receiving 300 mg olamkicept, and 50% (15/30) receiving placebo. The most common drug-related adverse events were bilirubin presence in the urine, hyperuricemia, and increased aspartate aminotransferase levels, and all were more common in the olamkicept groups compared with placebo.
Conclusions and relevance: Among patients with active ulcerative colitis, biweekly infusion of olamkicept 600 mg, but not 300 mg, resulted in a greater likelihood of clinical response at 12 weeks compared with placebo. Further research is needed for replication and to assess longer-term efficacy and safety.
Trial registration: ClinicalTrials.gov Identifier: NCT03235752.
Conflict of interest statement
Figures
References
-
- Ng SC, Tang W, Ching JY, et al. ; Asia–Pacific Crohn’s and Colitis Epidemiologic Study (ACCESS) Study Group . Incidence and phenotype of inflammatory bowel disease based on results from the Asia-Pacific Crohn’s and Colitis Epidemiology Study. Gastroenterology. 2013;145(1):158-165.e2. doi:10.1053/j.gastro.2013.04.007 - DOI - PubMed
-
- GBD 2017 Inflammatory Bowel Disease Collaborators . The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol Hepatol. 2020;5(1):17-30. doi:10.1016/S2468-1253(19)30333-4 - DOI - PMC - PubMed
