

Effect of Intrapartum Azithromycin vs Placebo on Neonatal Sepsis and Death: A Randomized Clinical Trial
- PMID: 36881034
- PMCID: PMC9993186
- DOI: 10.1001/jama.2022.24388
Effect of Intrapartum Azithromycin vs Placebo on Neonatal Sepsis and Death: A Randomized Clinical Trial
Abstract
Importance: Neonatal sepsis is a leading cause of neonatal mortality. New interventions are needed to decrease neonatal sepsis and mortality in regions with highest burden.
Objective: To evaluate the efficacy of intrapartum azithromycin to reduce neonatal sepsis or mortality, as well as neonatal and maternal infections.
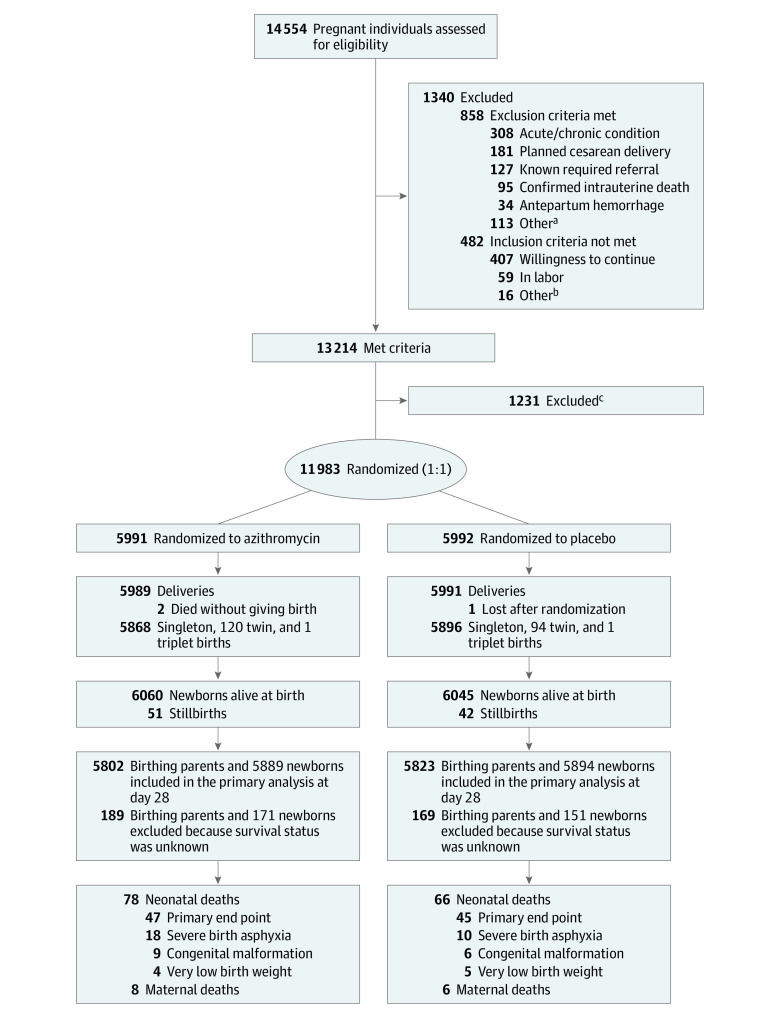
Design, setting, and participants: This double-blind, placebo-controlled, randomized clinical trial enrolled and followed up birthing parents and their infants at 10 health facilities in The Gambia and Burkina Faso, West Africa, between October 2017 and May 2021.
Interventions: Participants were assigned at random to receive oral azithromycin (2 g) or placebo (ratio 1:1) during labor.
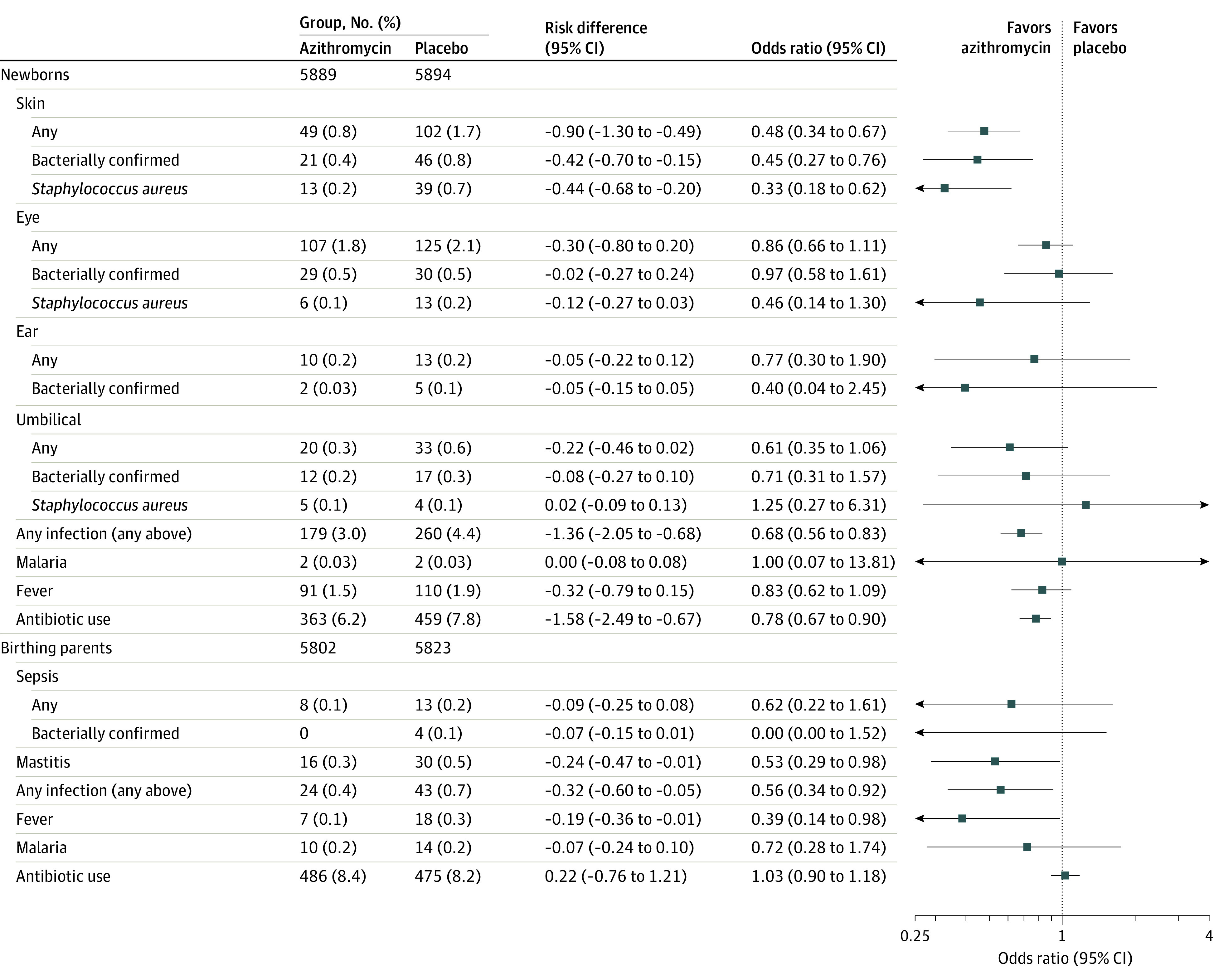
Main outcomes and measures: The primary outcome was a composite of neonatal sepsis or mortality, with the former defined based on microbiologic or clinical criteria. Secondary outcomes were neonatal infections (skin, umbilical, eye and ear infections), malaria, and fever; postpartum infections (puerperal sepsis, mastitis), fever, and malaria; and use of antibiotics during 4-week follow-up.
Results: The trial randomized 11 983 persons in labor (median age, 29.9 years). Overall, 225 newborns (1.9% of 11 783 live births) met the primary end point. The incidence of neonatal mortality or sepsis was similar in the azithromycin and placebo groups (2.0% [115/5889] vs 1.9% [110/5894]; risk difference [RD], 0.09 [95% CI, -0.39 to 0.57]), as was the incidence of neonatal mortality (0.8% vs 0.8%; RD, 0.04 [95% CI, -0.27 to 0.35]) and neonatal sepsis (1.3% vs 1.3%; RD, 0.02 [95% CI, -0.38 to 0.43]). Newborns in the azithromycin group compared with the placebo group had lower incidence of skin infections (0.8% vs 1.7%; RD, -0.90 [95% CI, -1.30 to -0.49]) and need for antibiotics (6.2% vs 7.8%; RD, -1.58 [95% CI, -2.49 to -0.67]). Postpartum parents in the azithromycin group had lower incidence of mastitis (0.3% vs 0.5%; RD, -0.24 [95% CI, -0.47 to -0.01]) and puerperal fever (0.1% vs 0.3%; RD, -0.19 [95% CI, -0.36 to -0.01]).
Conclusions and relevance: Azithromycin administered orally during labor did not reduce neonatal sepsis or mortality. These results do not support routine introduction of oral intrapartum azithromycin for this purpose.
Trial registration: ClinicalTrials.gov Identifier: NCT03199547.
Conflict of interest statement
Figures
Comment in
-
Still Looking for a Simple, Effective Prevention Measure for Neonatal Sepsis in High-Mortality Settings.JAMA. 2023 Mar 7;329(9):711-712. doi: 10.1001/jama.2022.24139. JAMA. 2023. PMID: 36881044 Free PMC article. No abstract available.
-
Intrapartum Azithromycin vs Placebo for Neonatal Sepsis.JAMA. 2023 Jul 11;330(2):187-188. doi: 10.1001/jama.2023.8328. JAMA. 2023. PMID: 37432437 No abstract available.
References
-
- Okomo U, Akpalu ENK, Le Doare K, et al. . Aetiology of invasive bacterial infection and antimicrobial resistance in neonates in sub-Saharan Africa: a systematic review and meta-analysis in line with the STROBE-NI reporting guidelines. Lancet Infect Dis. 2019;19(11):1219-1234. doi:10.1016/S1473-3099(19)30414-1 - DOI - PubMed
-
- Collaborators GBDU-M; GBD 2019 Under-5 Mortality Collaborators . Global, regional, and national progress towards Sustainable Development Goal 3.2 for neonatal and child health: all-cause and cause-specific mortality findings from the Global Burden of Disease Study 2019. Lancet. 2021;398(10303):870-905. doi:10.1016/S0140-6736(21)01207-1 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
