

Neonatal invasive candidiasis in low- and middle-income countries: Data from the NeoOBS study
- PMID: 36881725
- PMCID: PMC10026246
- DOI: 10.1093/mmy/myad010
Neonatal invasive candidiasis in low- and middle-income countries: Data from the NeoOBS study
Abstract
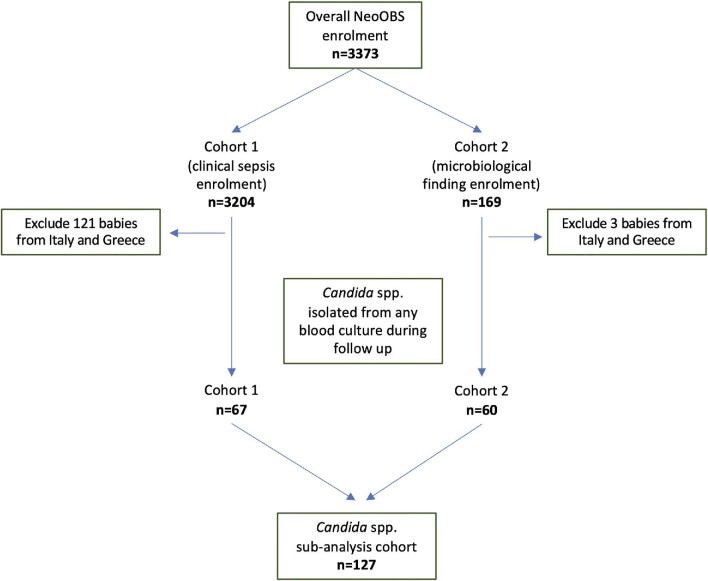
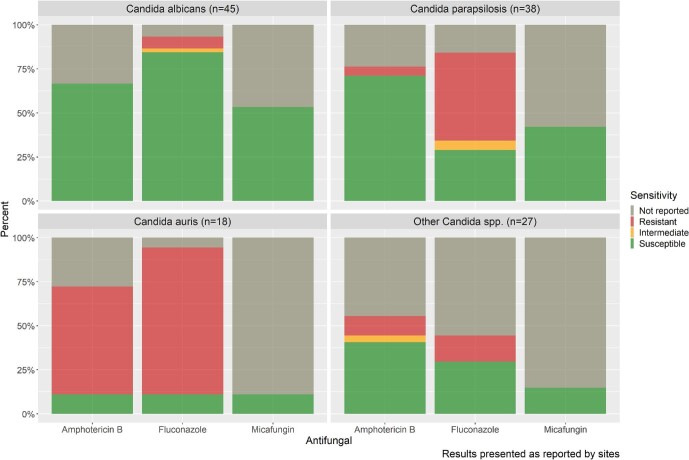
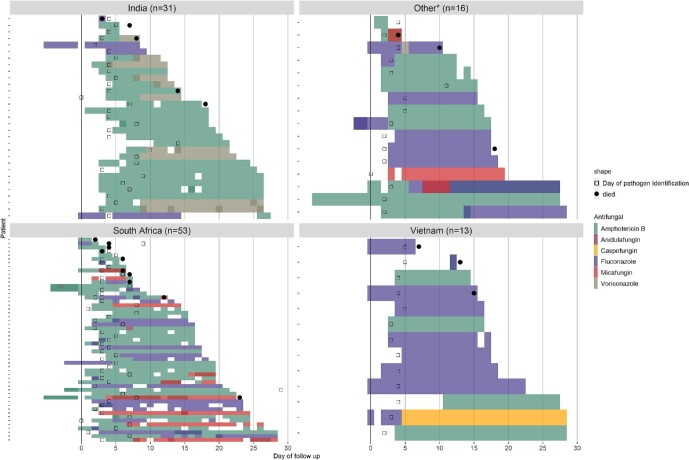
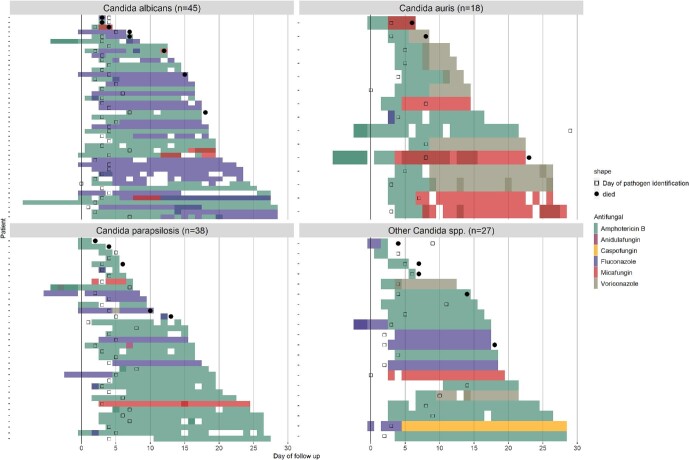
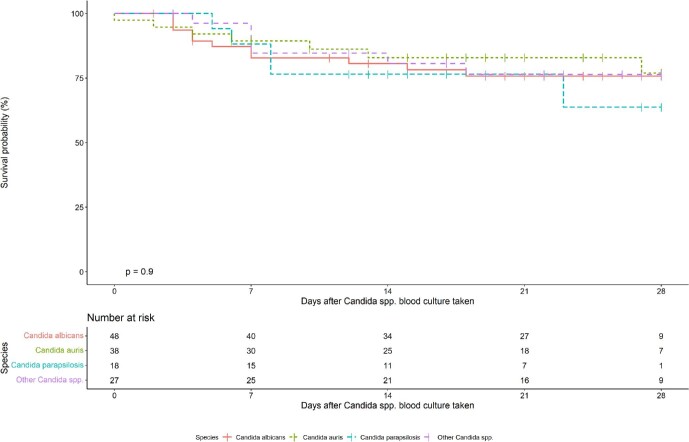
Neonatal invasive candidiasis (NIC) has significant morbidity and mortality. Reports have shown a different profile of those neonates affected with NIC and of fluconazole-resistant Candida spp. isolates in low- and middle-income countries (LMICs) compared to high-income countries (HICs). We describe the epidemiology, Candida spp. distribution, treatment, and outcomes of neonates with NIC from LMICs enrolled in a global, prospective, longitudinal, observational cohort study (NeoOBS) of hospitalized infants <60 days postnatal age with sepsis (August 2018-February 2021). A total of 127 neonates from 14 hospitals in 8 countries with Candida spp. isolated from blood culture were included. Median gestational age of affected neonates was 30 weeks (IQR: 28-34), and median birth weight was 1270 gr (interquartile range [IQR]: 990-1692). Only a minority had high-risk criteria, such as being born <28 weeks, 19% (24/127), or birth weight <1000 gr, 27% (34/127). The most common Candida species were C. albicans (n = 45, 35%), C. parapsilosis (n = 38, 30%), and Candida auris (n = 18, 14%). The majority of C. albicans isolates were fluconazole susceptible, whereas 59% of C. parapsilosis isolates were fluconazole-resistant. Amphotericin B was the most common antifungal used [74% (78/105)], followed by fluconazole [22% (23/105)]. Death by day 28 post-enrollment was 22% (28/127). To our knowledge, this is the largest multi-country cohort of NIC in LMICs. Most of the neonates would not have been considered at high risk for NIC in HICs. A substantial proportion of isolates was resistant to first choice fluconazole. Understanding the burden of NIC in LMIC is essential to guide future research and treatment guidelines.
Keywords: Candida auris; Candida parapsilosis; candidiasis; low- and middle-income countries; neonatal candidemia.
Plain language summary
Our study describes neonates from low- and middle-income countries with neonatal invasive candidiasis (NIC). Most of them were outside the groups considered at high risk for NIC described in high-income countries. Candida spp. epidemiology was also different. The mortality was high (22%). Further research in these settings is required.
© The Author(s) 2023. Published by Oxford University Press on behalf of The International Society for Human and Animal Mycology.
Conflict of interest statement
There are no conflicts of interest to declare.
Figures
References
-
- World Health Organization . Newborns: improving survival and well-being. World Health Organization. 2020. pp. 1–5.
-
- World Health Organization . Global report on the epidemiology and burden of sepsis: current evidence, identifying gaps and future directions. World Health Organization. 2020. p. 56, https://apps.who.int/iris/handle/10665/334216
-
- Benjamin DK, Stoll BJ, Fanaroff AAet al. Neonatal candidiasis among extremely low birth weight infants: risk factors, mortality rates, and neurodevelopmental outcomes at 18 to 22 months. Pediatrics. 2006; 117: 84–92. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
