

Patterns of utilisation of specialist care after SARS-Cov-2 infection: a retrospective cohort study
- PMID: 36882238
- PMCID: PMC10008201
- DOI: 10.1136/bmjopen-2022-063493
Patterns of utilisation of specialist care after SARS-Cov-2 infection: a retrospective cohort study
Abstract
Objective: To explore the pattern of health services utilisation of people who had had a documented SARS-Cov-2 infection.
Design: Retrospective cohort study.
Setting: The Italian province of Reggio Emilia.
Participants: 36 036 subjects who recovered from SARS-CoV-2 infection during the period September 2020-May 2021. These were matched for age, sex and Charlson Index with an equal number of subjects never found positive at the SARS-Cov-2 swab test over the study period.
Main outcome measures: Hospital admissions for all medical conditions and for respiratory or cardiovascular conditions only; access to emergency room (for any cause); outpatient specialist visits (pneumology, cardiology, neurology, endocrinology, gastroenterology, rheumatology, dermatology, mental health) and overall cost of care.
Results:
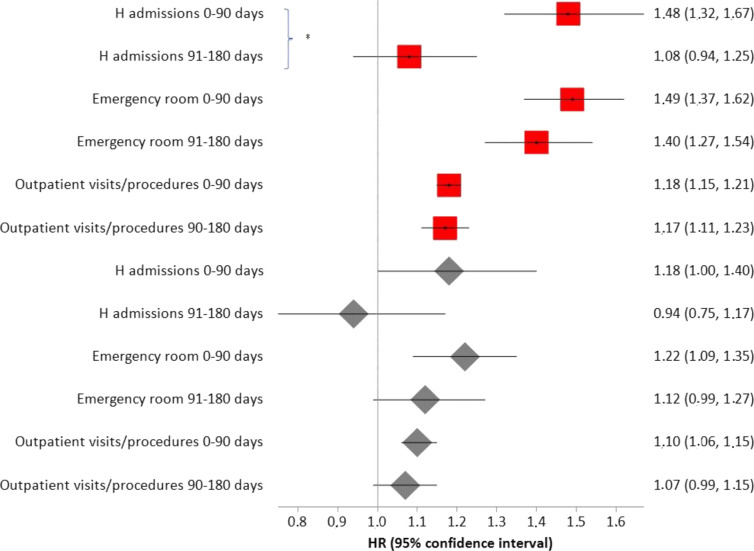
Within a median follow-up time of 152 days (range 1-180), previous exposure to SARS-Cov-2 infection was always associated with higher probability of needing access to hospital or ambulatory care, except for dermatology, mental health and gastroenterology specialist visits. Post-COVID subjects with Charlson Index≥1 were hospitalised more frequently for heart disease and for non-surgical reasons than subjects with Charlson index=0, whereas the opposite occurred for hospitalisations for respiratory diseases and pneumology visits. A previous SARS-CoV-2 infection was associated with 27% higher cost of care compared with people never infected. The difference in cost was more evident among those with Charlson Index
Conclusions: Our findings reflect the burden of post-COVID sequelae, providing some specific insight on their impact on the extra-use of health services according to patients' characteristics and vaccination status. Vaccination is associated with lower cost of care following SARS-CoV-2 infection, highlighting the favourable impact of vaccines on the use of health services even when they do not prevent infection.
Keywords: COVID-19; Clinical governance; EPIDEMIOLOGY; Organisation of health services; PUBLIC HEALTH.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- World Health Organization . A clinical case definition of post COVID-19 condition by A delphi consensus. 2021. Available: www.who.int/publications/i/item/WHO-2019-nCoV-Post_COVID-19_condition-Cl...
-
- National Institute for Health and Care Excellence (NICE), Scottish Intercollegiate Guidelines Network (SIGN), Royal College of General Practitioners (RCGP) . COVID-19 rapid guideline: managing the long-term effects of COVID-19. n.d. Available: www.nice.org.uk/guidance/ng188/resources/covid19-rapid-guideline-managin...
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous