

Trimethylamine N-oxide is associated with long-term mortality risk: the multi-ethnic study of atherosclerosis
- PMID: 36883587
- PMCID: PMC10411925
- DOI: 10.1093/eurheartj/ehad089
Trimethylamine N-oxide is associated with long-term mortality risk: the multi-ethnic study of atherosclerosis
Abstract
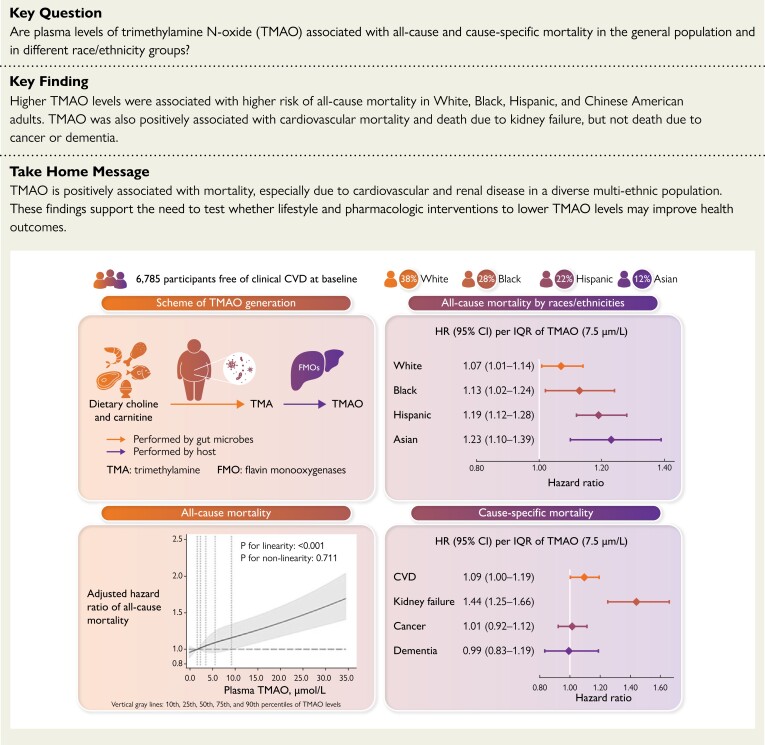
Aims: Little is known about associations of trimethylamine N-oxide (TMAO), a novel gut microbiota-generated metabolite of dietary phosphatidylcholine and carnitine, and its changes over time with all-cause and cause-specific mortality in the general population or in different race/ethnicity groups. The study aimed to investigate associations of serially measured plasma TMAO levels and changes in TMAO over time with all-cause and cause-specific mortality in a multi-ethnic community-based cohort.
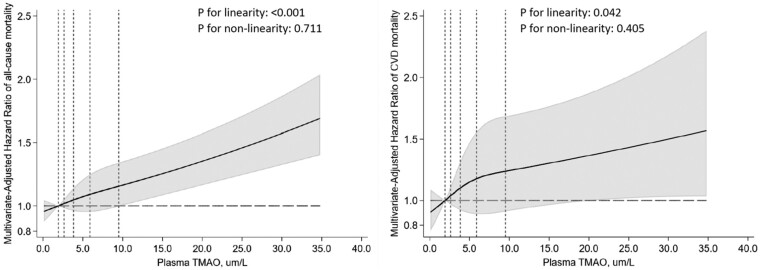
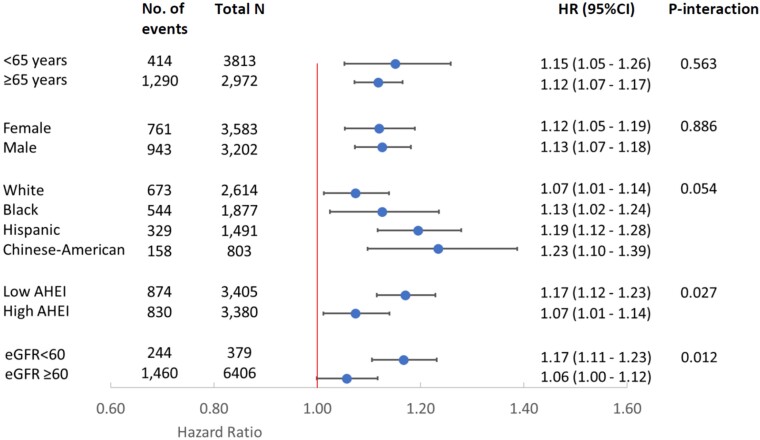
Methods and results: The study included 6,785 adults from the Multi-Ethnic Study of Atherosclerosis. TMAO was measured at baseline and year 5 using mass spectrometry. Primary outcomes were adjudicated all-cause mortality and cardiovascular disease (CVD) mortality. Secondary outcomes were deaths due to kidney failure, cancer, or dementia obtained from death certificates. Cox proportional hazards models with time-varying TMAO and covariates assessed the associations with adjustment for sociodemographics, lifestyles, diet, metabolic factors, and comorbidities. During a median follow-up of 16.9 years, 1704 participants died and 411 from CVD. Higher TMAO levels associated with higher risk of all-cause mortality [hazard ratio (HR): 1.12, 95% confidence interval (CI): 1.08-1.17], CVD mortality (HR: 1.09, 95% CI: 1.00-1.09), and death due to kidney failure (HR: 1.44, 95% CI: 1.25-1.66) per inter-quintile range, but not deaths due to cancer or dementia. Annualized changes in TMAO levels associated with higher risk of all-cause mortality (HR: 1.10, 95% CI: 1.05-1.14) and death due to kidney failure (HR: 1.54, 95% CI: 1.26-1.89) but not other deaths.
Conclusion: Plasma TMAO levels were positively associated with mortality, especially deaths due to cardiovascular and renal disease, in a multi-ethnic US cohort.
Keywords: Cardiovascular disease; Microbiome; Mortality; Red meat; Trimethylamine N-oxide.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
Conflict of interest Z.W. and S.L.H. report being named as co-inventor on pending and issued patents held by the Cleveland Clinic relating to cardiovascular diagnostics and therapeutics. S.L.H. also reports being a paid consultant for Zehna Therapeutics. S.L.H. reports having received research funds from Procter & Gamble, Zehna Therapeutics and Roche Diagnostics. Z.W. and S.L.H. report being eligible to receive royalty payments for inventions or discoveries related to cardiovascular diagnostics or therapeutics from Cleveland Heart Lab, and Procter & Gamble, and S.L.H. from Zehna Therapeutics. B.M.P. serves on the Steering Committee of the Yale Open Data Access Project funded by Johnson & Johnson. D. Mozaffarian reports research funding from the National Institutes of Health, the Gates Foundation, The Rockefeller Foundation, Vail Innovative Global Research, and Kaiser Permanente; personal fees from Acasti Pharma and Barilla; scientific advisory board, Beren Therapeutics, Brightseed, Calibrate, Elysium Health, Filtricine, HumanCo, Instacart, January Inc, Perfect Day, Tiny Organics, and (ended) Discern Dx, Day Two, and Season Health; stock ownership in Calibrate and HumanCo; and chapter royalties from UpToDate. The other authors report no relationships with industry.
Figures
Comment in
-
They eat what we eat, they digest what we ingest.Eur Heart J. 2023 May 7;44(18):1619-1621. doi: 10.1093/eurheartj/ehad104. Eur Heart J. 2023. PMID: 36905155 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
- N01 HC095168/HL/NHLBI NIH HHS/United States
- R01HL135920/NH/NIH HHS/United States
- P01 HL147823/HL/NHLBI NIH HHS/United States
- 75N92020D00001/HL/NHLBI NIH HHS/United States
- R01 HL103866/HL/NHLBI NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- R01 HL135920/HL/NHLBI NIH HHS/United States
- N01HC95159/HL/NHLBI NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- N01 HC095166/HL/NHLBI NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
- 75N92020D00002/HL/NHLBI NIH HHS/United States
- HHSN268201500003C/HL/NHLBI NIH HHS/United States
- N01 HC095161/HL/NHLBI NIH HHS/United States
- 75N92020D00005/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- 75N92020D00003/HL/NHLBI NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- 75N92020D00004/HL/NHLBI NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- 75N92020D00007/HL/NHLBI NIH HHS/United States
- UL1-TR-000040/HL/NHLBI NIH HHS/United States
- HHSN268201500003I/HL/NHLBI NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- 75N92020D00006/HL/NHLBI NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
