

The Bidirectional Gut-Lung Axis in Chronic Obstructive Pulmonary Disease
- PMID: 36883945
- PMCID: PMC10161745
- DOI: 10.1164/rccm.202206-1066TR
The Bidirectional Gut-Lung Axis in Chronic Obstructive Pulmonary Disease
Abstract
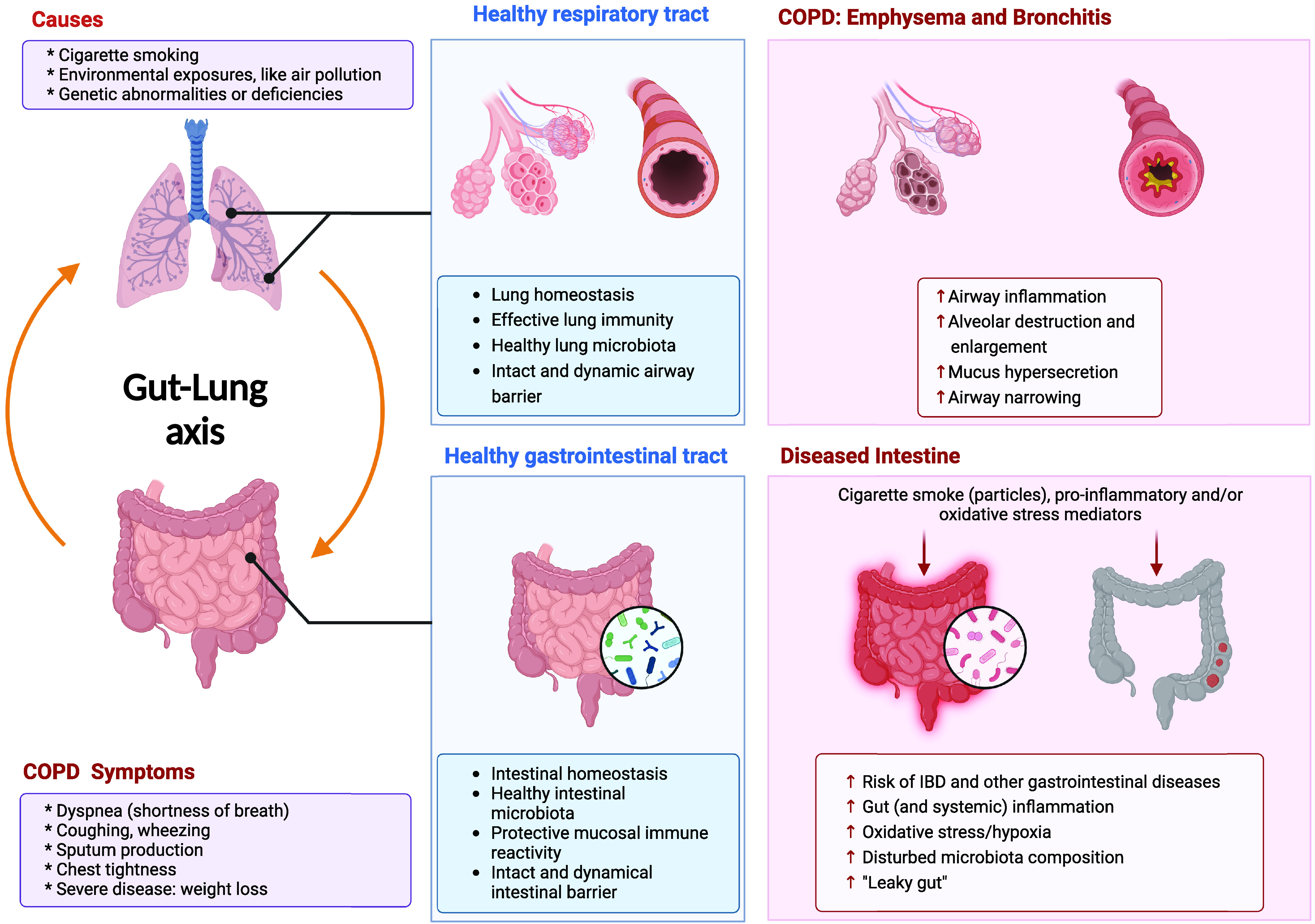
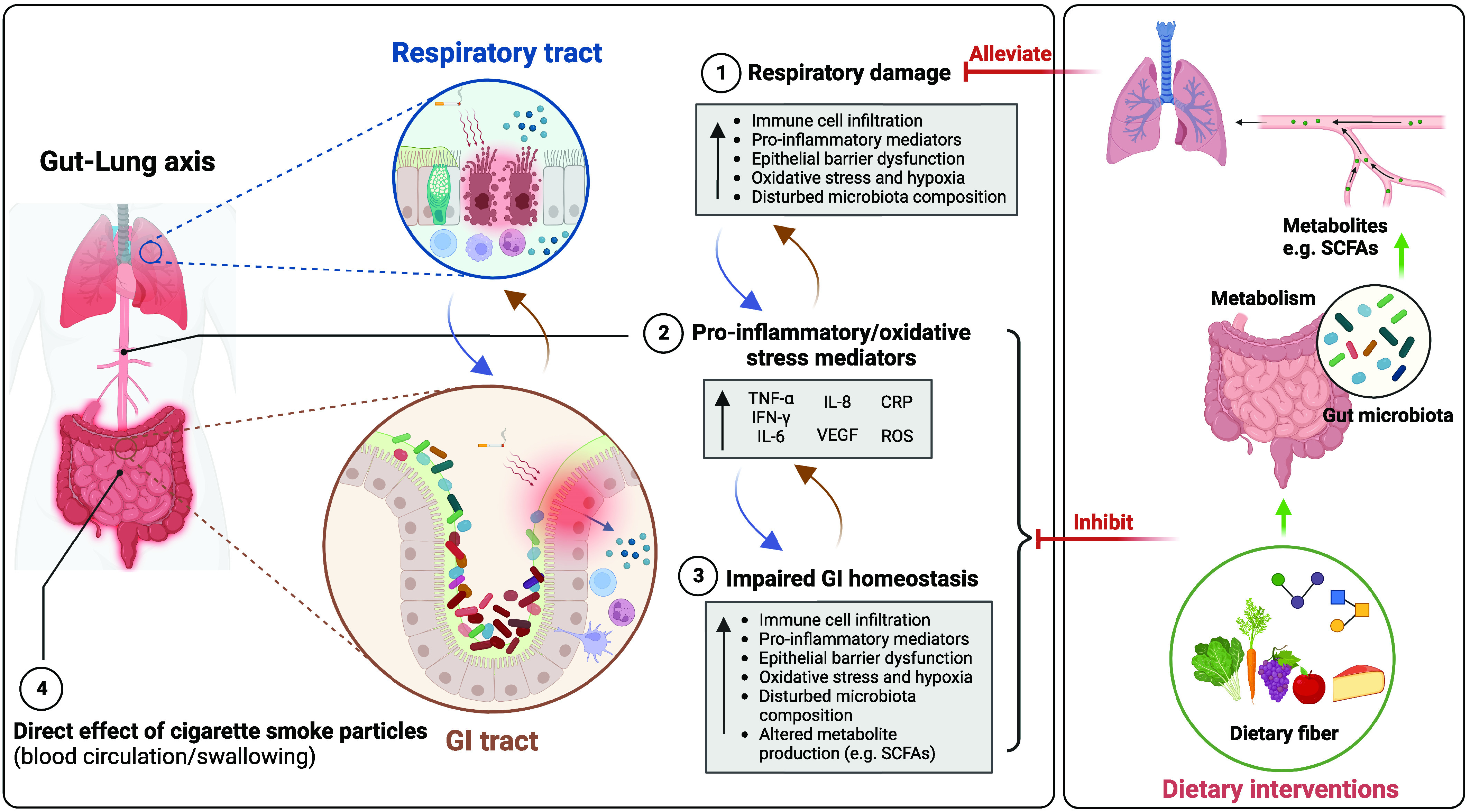
Epidemiological studies indicate that chronic obstructive pulmonary disease (COPD) is associated with the incidence of changes in intestinal health. Cigarette smoking, as one of the major causes of COPD, can have an impact on the gastrointestinal system and promotes intestinal diseases. This points to the existence of gut-lung interactions, but an overview of the underlying mechanisms of the bidirectional connection between the lungs and the gut in COPD is lacking. The interaction between the lungs and the gut can occur through circulating inflammatory cells and mediators. Moreover, gut microbiota dysbiosis, observed in both COPD and intestinal disorders, can lead to a disturbed mucosal environment, including the intestinal barrier and immune system, and hence may negatively affect both the gut and the lungs. Furthermore, systemic hypoxia and oxidative stress that occur in COPD may also be involved in intestinal dysfunction and play a role in the gut-lung axis. In this review, we summarize data from clinical research, animal models, and in vitro studies that may explain the possible mechanisms of gut-lung interactions associated with COPD. Interesting observations on the possibility of promising future add-on therapies for intestinal dysfunction in patients with COPD are highlighted.
Keywords: gut–lung axis; hypoxia; lung diseases; microbiota; systemic inflammation.
Figures
Comment in
-
Gut Microbiota Dysbiosis and Chronic Obstructive Pulmonary Disease: A Question of Chicken and Egg.Am J Respir Crit Care Med. 2023 Dec 1;208(11):1238-1240. doi: 10.1164/rccm.202307-1285LE. Am J Respir Crit Care Med. 2023. PMID: 37672767 Free PMC article. No abstract available.
Similar articles
-
Imbalance of gut microbiota is involved in the development of chronic obstructive pulmonary disease: A review.Biomed Pharmacother. 2023 Sep;165:115150. doi: 10.1016/j.biopha.2023.115150. Epub 2023 Jul 8. Biomed Pharmacother. 2023. PMID: 37429232 Review.
-
Links Between Inflammatory Bowel Disease and Chronic Obstructive Pulmonary Disease.Front Immunol. 2020 Sep 11;11:2144. doi: 10.3389/fimmu.2020.02144. eCollection 2020. Front Immunol. 2020. PMID: 33042125 Free PMC article. Review.
-
The role and mechanism of gut-lung axis mediated bidirectional communication in the occurrence and development of chronic obstructive pulmonary disease.Gut Microbes. 2024 Jan-Dec;16(1):2414805. doi: 10.1080/19490976.2024.2414805. Epub 2024 Oct 24. Gut Microbes. 2024. PMID: 39446051 Free PMC article. Review.
-
Gut Microbiome as a Possible Cause of Occurrence and Therapeutic Target in Chronic Obstructive Pulmonary Disease.J Microbiol Biotechnol. 2023 Sep 28;33(9):1111-1118. doi: 10.4014/jmb.2301.01033. Epub 2023 Mar 30. J Microbiol Biotechnol. 2023. PMID: 37164760 Free PMC article. Review.
-
Lung microbiome, gut-lung axis and chronic obstructive pulmonary disease.Curr Opin Pulm Med. 2022 Mar 1;28(2):134-138. doi: 10.1097/MCP.0000000000000853. Curr Opin Pulm Med. 2022. PMID: 34907959 Review.
Cited by
-
Effects of probiotic treatment on patients and animals with chronic obstructive pulmonary disease: a systematic review and meta-analysis of randomized control trials.Front Cell Infect Microbiol. 2024 Sep 11;14:1411222. doi: 10.3389/fcimb.2024.1411222. eCollection 2024. Front Cell Infect Microbiol. 2024. PMID: 39324058 Free PMC article.
-
Genetic and observational associations of lung function with gastrointestinal tract diseases: pleiotropic and mendelian randomization analysis.Respir Res. 2023 Dec 15;24(1):315. doi: 10.1186/s12931-023-02621-0. Respir Res. 2023. PMID: 38102678 Free PMC article.
-
COVID-19 influenced gut dysbiosis, post-acute sequelae, immune regulation, and therapeutic regimens.Front Cell Infect Microbiol. 2024 May 28;14:1384939. doi: 10.3389/fcimb.2024.1384939. eCollection 2024. Front Cell Infect Microbiol. 2024. PMID: 38863829 Free PMC article. Review.
-
Distinct enterotypes and dysbiosis: unraveling gut microbiota in pulmonary and critical care medicine inpatients.Respir Res. 2024 Aug 10;25(1):304. doi: 10.1186/s12931-024-02943-7. Respir Res. 2024. PMID: 39127664 Free PMC article.
-
Microbial Buffer? The Human Lung Microbiome and Immune Responses to Diesel Exhaust.Environ Health Perspect. 2024 Jul;132(7):74002. doi: 10.1289/EHP15252. Epub 2024 Jul 29. Environ Health Perspect. 2024. PMID: 39073991 Free PMC article.
References
-
- Rutten EP, Spruit MA, Franssen FM, Buurman WA, Wouters EF, Lenaerts K. GI symptoms in patients with COPD. Chest . 2014;145:1437–1438. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
