

Association between computed tomography perfusion and the effect of intravenous alteplase prior to endovascular treatment in acute ischemic stroke
- PMID: 36884080
- PMCID: PMC10169898
- DOI: 10.1007/s00234-023-03139-4
Association between computed tomography perfusion and the effect of intravenous alteplase prior to endovascular treatment in acute ischemic stroke
Abstract
Purpose: Intravenous alteplase (IVT) prior to endovascular treatment (EVT) is neither superior nor noninferior to EVT alone in acute ischemic stroke patients. We aim to assess whether the effect of IVT prior to EVT differs according to CT perfusion (CTP)-based imaging parameters.
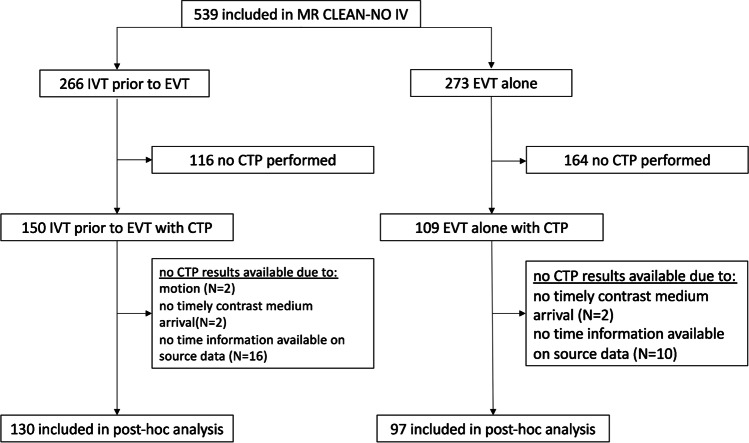
Methods: In this retrospective post hoc analysis, we included patients from the MR CLEAN-NO IV with available CTP data. CTP data were processed using syngo.via (version VB40). We performed multivariable logistic regression to obtain the effect size estimates (adjusted common odds ratio a[c]OR) on 90-day functional outcome (modified Rankin Scale [mRS]) and functional independence (mRS 0-2) for CTP parameters with two-way multiplicative interaction terms between IVT administration and the studied parameters.
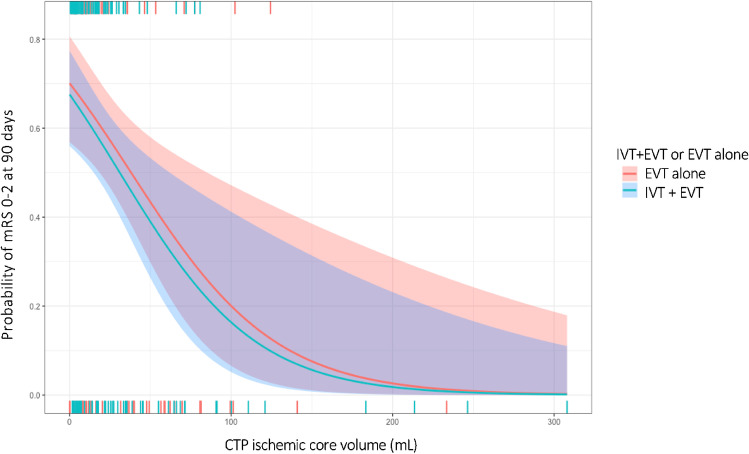
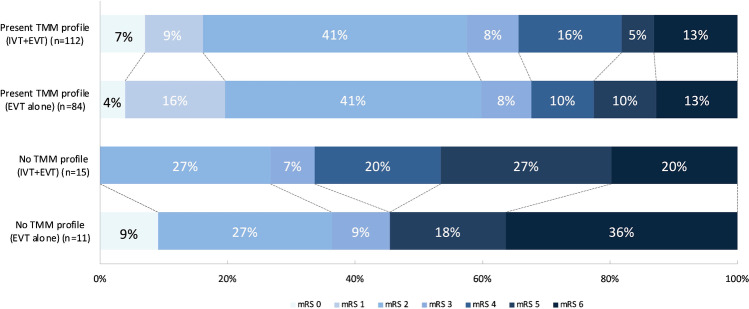
Results: In 227 patients, median CTP-estimated core volume was 13 (IQR 5-35) mL. The treatment effect of IVT prior to EVT on outcome was not altered by CTP-estimated ischemic core volume, penumbral volume, mismatch ratio, and presence of a target mismatch profile. None of the CTP parameters was significantly associated with functional outcome after adjusting for confounders.
Conclusion: In directly admitted patients with limited CTP-estimated ischemic core volumes who presented within 4.5 h after symptom onset, CTP parameters did not statistically significantly alter the treatment effect of IVT prior to EVT. Further studies are needed to confirm these results in patients with larger core volumes and more unfavorable baseline perfusion profiles on CTP imaging.
Keywords: Alteplase; CT perfusion; Ischemic core; Stroke; Thrombectomy.
© 2023. The Author(s).
Conflict of interest statement
BJE reports grants from LtC (ZonMW and TKI-PPP of Health Holland) outside the submitted work. CBLMM reports grants from CVON/Dutch Heart Foundation and Stryker (related) and TWIN Foundation, European Commission and Health Evaluation Netherlands, outside the submitted work, all paid to institution, and is (minority interest) shareholder of Nicolab. YBWEM reports grants from the Dutch Heart Foundation, Brain Foundation Netherlands, and Stryker outside the submitted work (paid to institution) and is shareholder of Nicolab. AL reports grants from Dutch Heart Foundation, the Brain Foundation Netherlands, Health-Holland, Stryker, Medtronic, Penumbra, Cerenovus, Siemens Healthineers, Philips Healthcare, and GE Healthcare, all paid to institution. HAM is co-founder and shareholder of Nicolab. All other contributors report no conflicts of interest.
Figures
Similar articles
-
Penumbral imaging and functional outcome in patients with anterior circulation ischaemic stroke treated with endovascular thrombectomy versus medical therapy: a meta-analysis of individual patient-level data.Lancet Neurol. 2019 Jan;18(1):46-55. doi: 10.1016/S1474-4422(18)30314-4. Epub 2018 Nov 6. Lancet Neurol. 2019. PMID: 30413385
-
Bridging Thrombolysis Before Endovascular Therapy in Stroke Patients With Faster Core Growth.Neurology. 2023 May 16;100(20):e2083-e2092. doi: 10.1212/WNL.0000000000207154. Epub 2023 Mar 24. Neurology. 2023. PMID: 36963842 Free PMC article.
-
Endovascular Thrombectomy Outcomes with and without Intravenous Thrombolysis for Large Ischemic Cores Identified with CT or MRI.Radiology. 2023 Oct;309(1):e230440. doi: 10.1148/radiol.230440. Radiology. 2023. PMID: 37847131
-
Clinical Relevance of Computed Tomography Perfusion-Estimated Infarct Volume in Acute Ischemic Stroke Patients within the 6-h Therapeutic Time Window.Cerebrovasc Dis. 2022;51(4):438-446. doi: 10.1159/000519901. Epub 2022 Jan 21. Cerebrovasc Dis. 2022. PMID: 35066495
-
Efficacy and safety of endovascular treatment with or without intravenous alteplase in acute anterior circulation large vessel occlusion stroke: a meta-analysis of randomized controlled trials.Neurol Sci. 2022 Jun;43(6):3551-3563. doi: 10.1007/s10072-022-06017-8. Epub 2022 Mar 22. Neurol Sci. 2022. PMID: 35314911 Review.
Cited by
-
Automated advanced imaging in acute ischemic stroke. Certainties and uncertainties.Eur J Radiol Open. 2023 Sep 20;11:100524. doi: 10.1016/j.ejro.2023.100524. eCollection 2023 Dec. Eur J Radiol Open. 2023. PMID: 37771657 Free PMC article.
References
-
- Mitchell PJ, Yan B, Churilov L, et al. Endovascular thrombectomy versus standard bridging thrombolytic with endovascular thrombectomy within 4·5 h of stroke onset: an open-label, blinded-endpoint, randomised non-inferiority trial. Lancet (London, England) 2022;400:116–125. doi: 10.1016/S0140-6736(22)00564-5. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
