

Human germline heterozygous gain-of-function STAT6 variants cause severe allergic disease
- PMID: 36884218
- PMCID: PMC10037107
- DOI: 10.1084/jem.20221755
Human germline heterozygous gain-of-function STAT6 variants cause severe allergic disease
Abstract
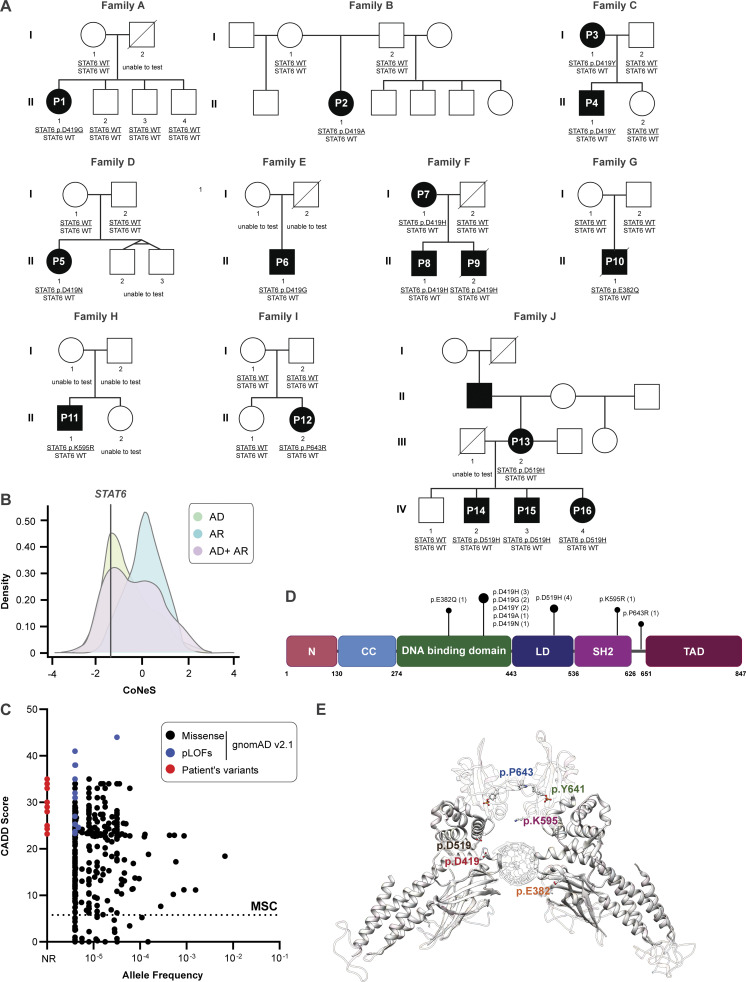
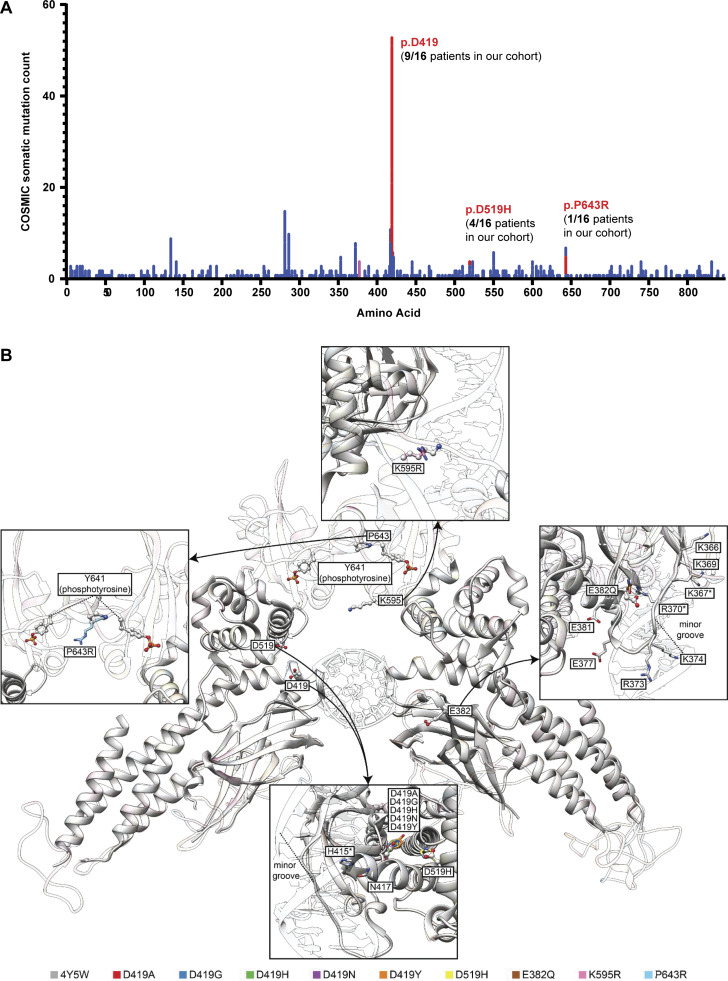
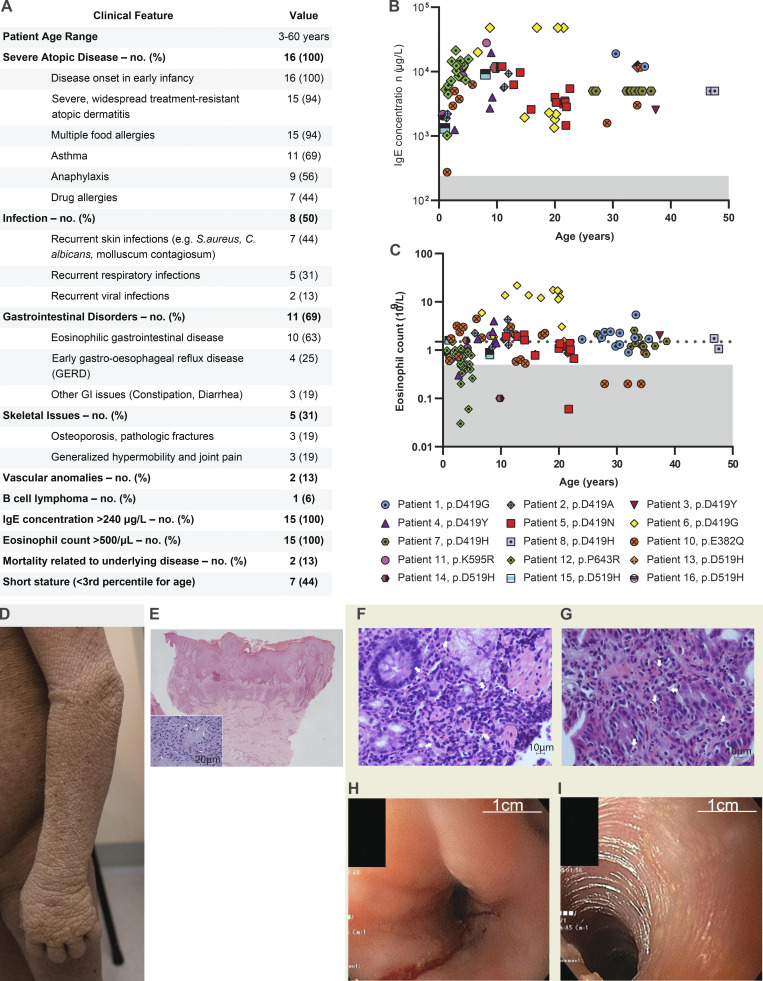
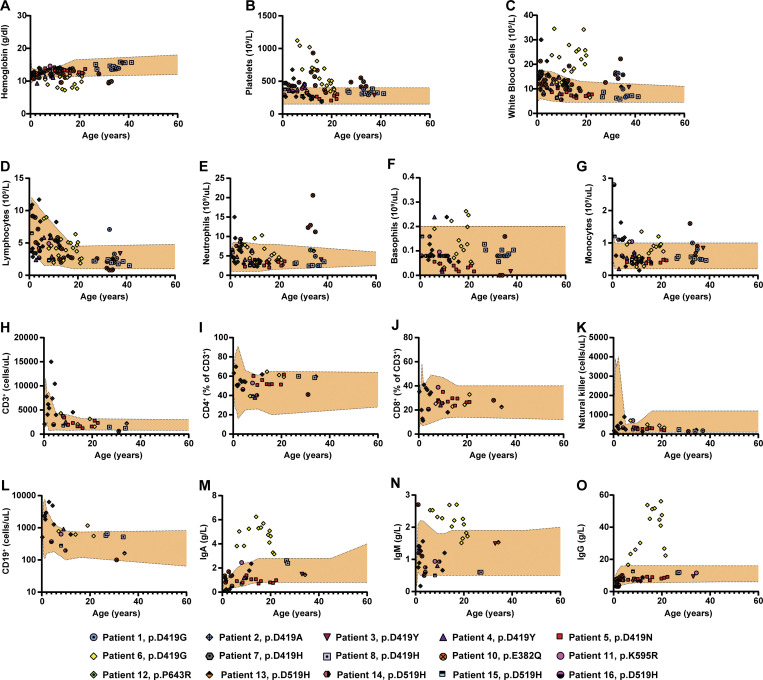
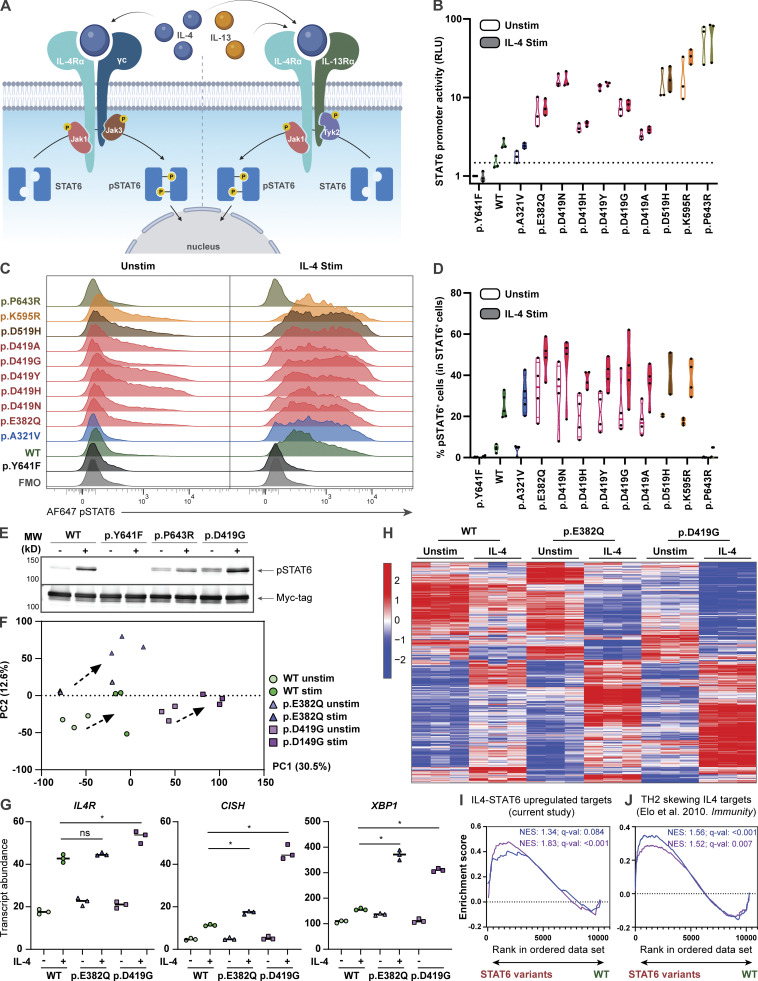
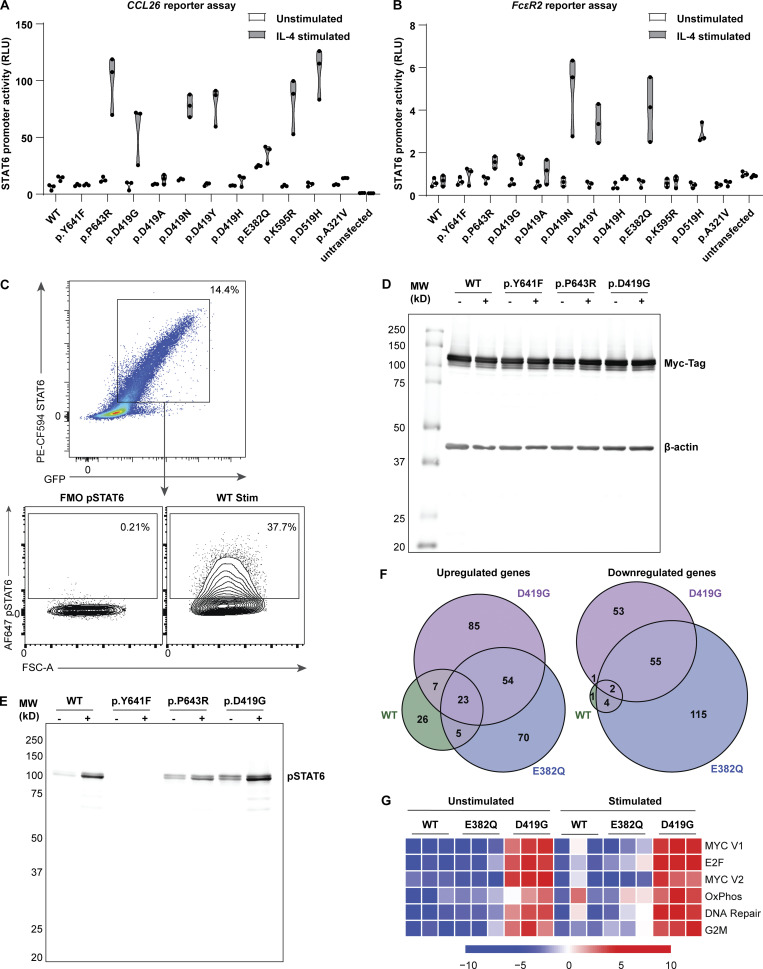
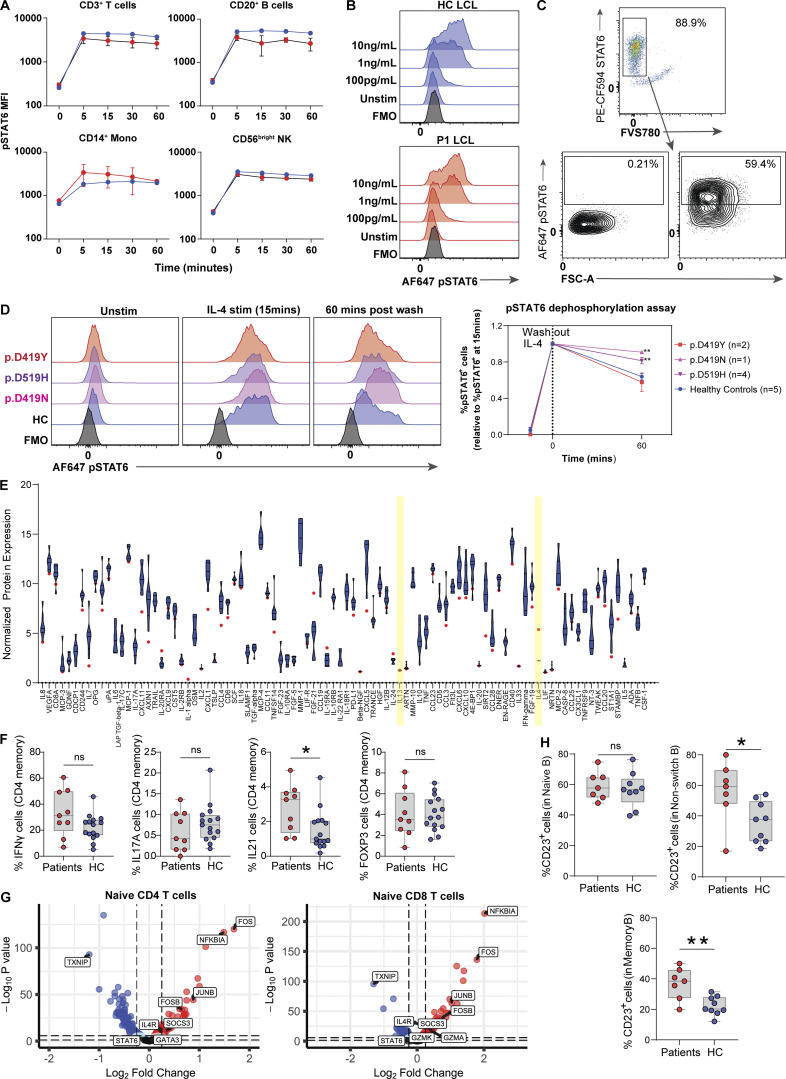
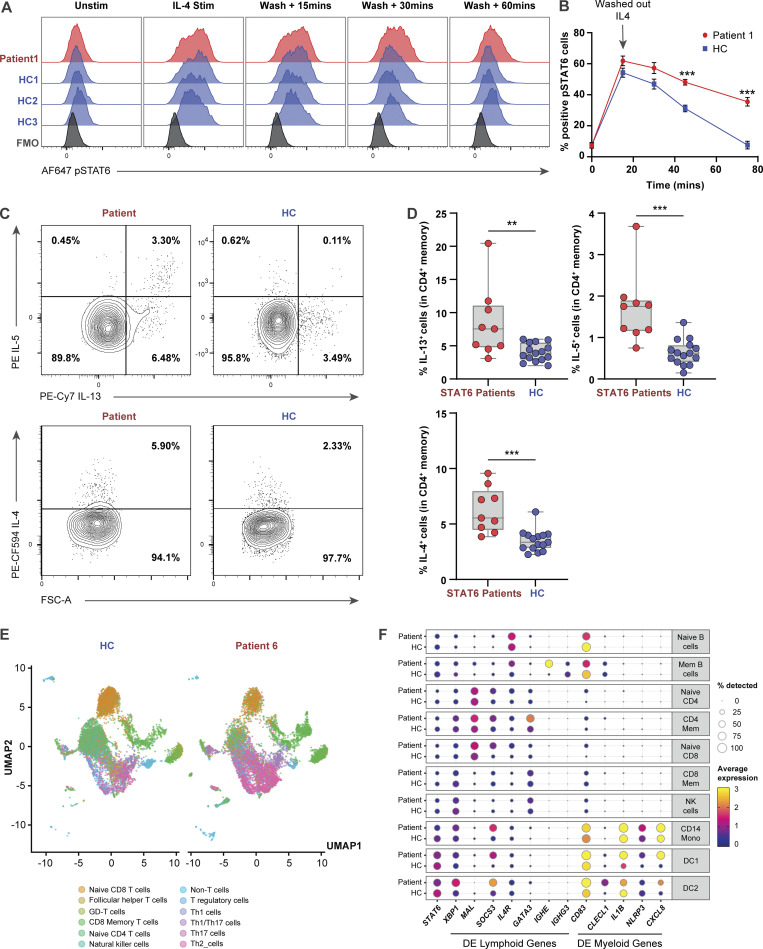
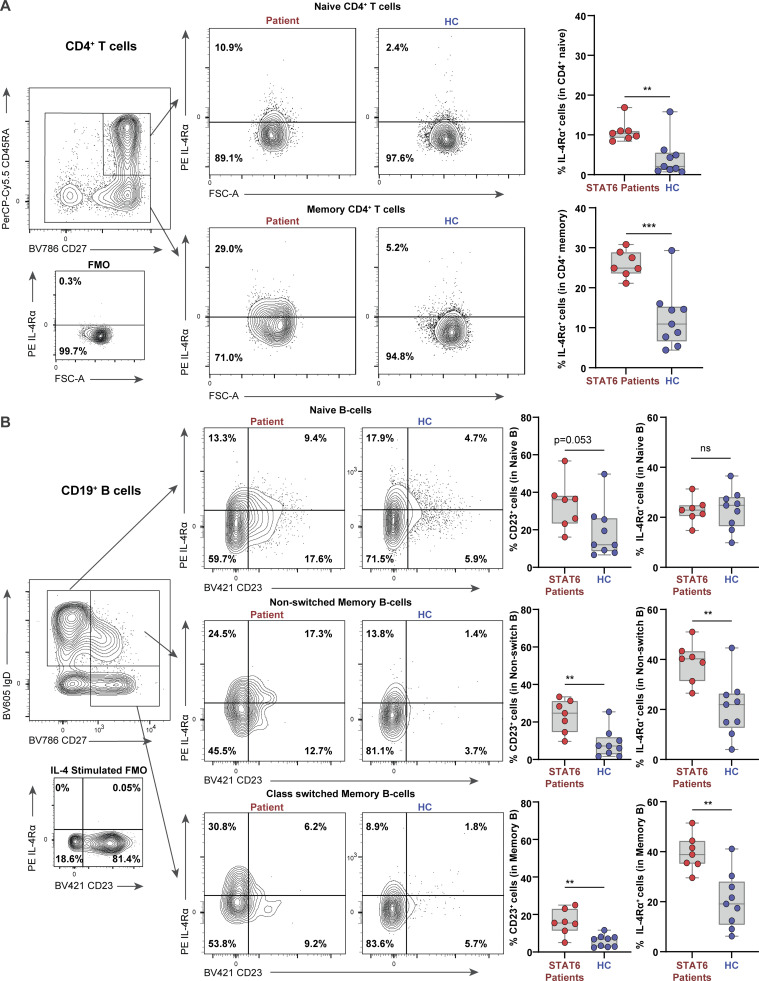
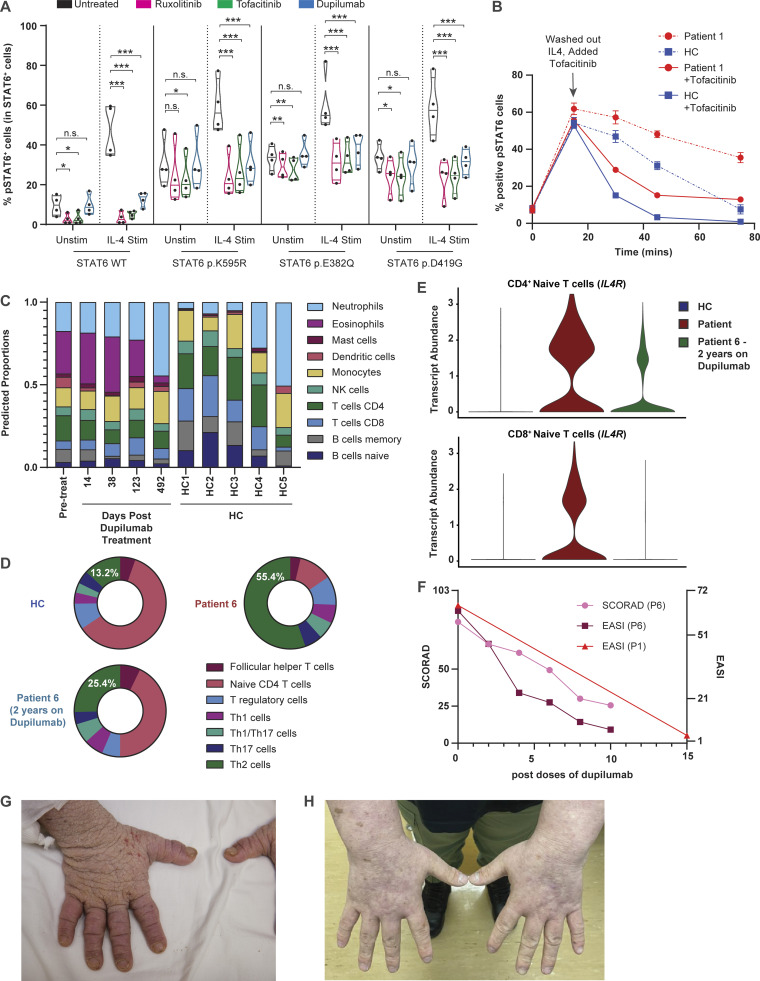
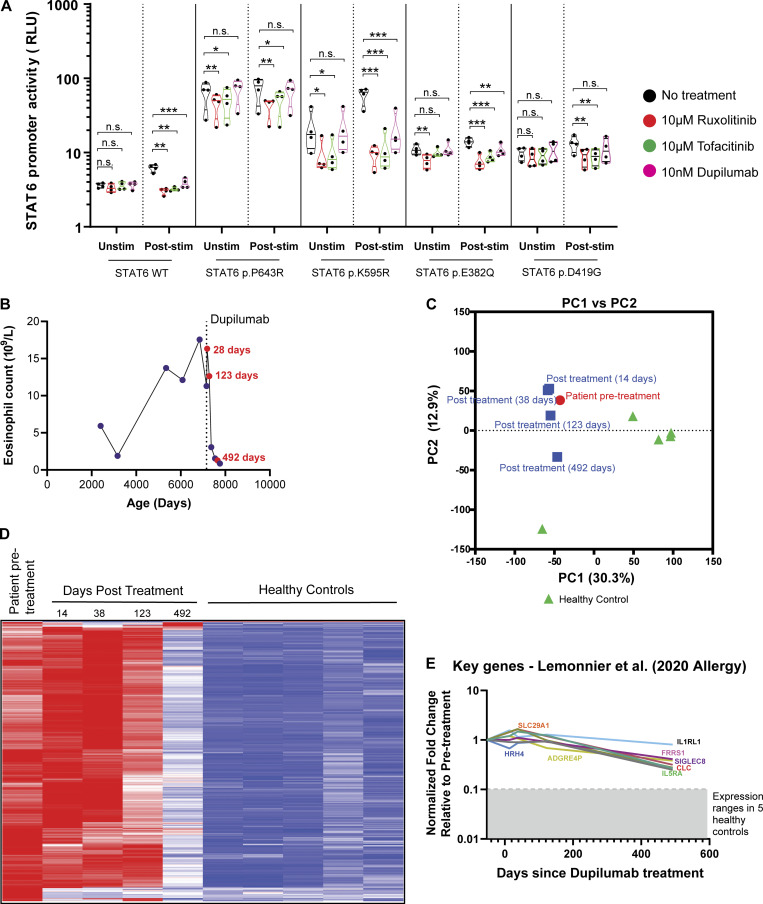
STAT6 (signal transducer and activator of transcription 6) is a transcription factor that plays a central role in the pathophysiology of allergic inflammation. We have identified 16 patients from 10 families spanning three continents with a profound phenotype of early-life onset allergic immune dysregulation, widespread treatment-resistant atopic dermatitis, hypereosinophilia with esosinophilic gastrointestinal disease, asthma, elevated serum IgE, IgE-mediated food allergies, and anaphylaxis. The cases were either sporadic (seven kindreds) or followed an autosomal dominant inheritance pattern (three kindreds). All patients carried monoallelic rare variants in STAT6 and functional studies established their gain-of-function (GOF) phenotype with sustained STAT6 phosphorylation, increased STAT6 target gene expression, and TH2 skewing. Precision treatment with the anti-IL-4Rα antibody, dupilumab, was highly effective improving both clinical manifestations and immunological biomarkers. This study identifies heterozygous GOF variants in STAT6 as a novel autosomal dominant allergic disorder. We anticipate that our discovery of multiple kindreds with germline STAT6 GOF variants will facilitate the recognition of more affected individuals and the full definition of this new primary atopic disorder.
© 2023 Sharma et al.
Conflict of interest statement
Disclosures: S. Delafontaine is supported by the Personal Research Foundation Flanders grant 11F4421N. T.F. Brown-Whitehorn reported grants from DBV Technology, “other” from DBV Technology, and grants from Regeneron outside the submitted work. J.R. Treat reported personal fees from Sanofi/Regeneron outside the submitted work. D. Bullens reported grants from Research Foundation Flanders and Sanofi Genzyme outside the submitted work. E.C. Morris reported personal fees from Quell Therapeutics Limited outside the submitted work. J.J. O’Shea reported a patent for Janus kinase inhibitors with royalties paid (National Institutes of Health). P. Palma reported grants from the ViiV Foundation and Chiesi Foundation outside the submitted work. S.O. Burns has received grant support from CSL Behring and personal fees or travel expenses from CSL Behring, Baxalta US Inc, Glaxo Smith Kline, and Biotest. I. Meyts reported grants from CSLBehring (paid to institution) and “other” from Boehringer-Ingelheim SAB (paid to institution) outside the submitted work. J. Heimall reported grants from Regeneron, CSL Behring, Enzyvant, and ADMA; and personal fees from CSL Behring, UpToDate, Enzyvant, ADMA, and CIRM outside the submitted work. No other disclosures were reported.
Figures
Comment in
-
Learning while treating: Gain-of-function STAT6 variants in severe allergic disease.Cell Rep Med. 2023 May 16;4(5):101040. doi: 10.1016/j.xcrm.2023.101040. Cell Rep Med. 2023. PMID: 37196636 Free PMC article.
References
-
- Astle, W.J., Elding H., Jiang T., Allen D., Ruklisa D., Mann A.L., Mead D., Bouman H., Riveros-Mckay F., Kostadima M.A., et al. . 2016. The allelic landscape of human blood cell trait variation and links to common complex disease. Cell. 167:1415–1429.e19. 10.1016/j.cell.2016.10.042 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
