

Nirogacestat, a γ-Secretase Inhibitor for Desmoid Tumors
- PMID: 36884323
- PMCID: PMC11225596
- DOI: 10.1056/NEJMoa2210140
Nirogacestat, a γ-Secretase Inhibitor for Desmoid Tumors
Update in
-
A study to learn if nirogacestat works and is safe for adult participants with desmoid tumors: a plain language summary of the DeFi study.Future Oncol. 2025 Apr;21(8):889-901. doi: 10.1080/14796694.2025.2462519. Epub 2025 Mar 12. Future Oncol. 2025. PMID: 40070345 Free PMC article.
Abstract
Background: Desmoid tumors are rare, locally aggressive, highly recurrent soft-tissue tumors without approved treatments.
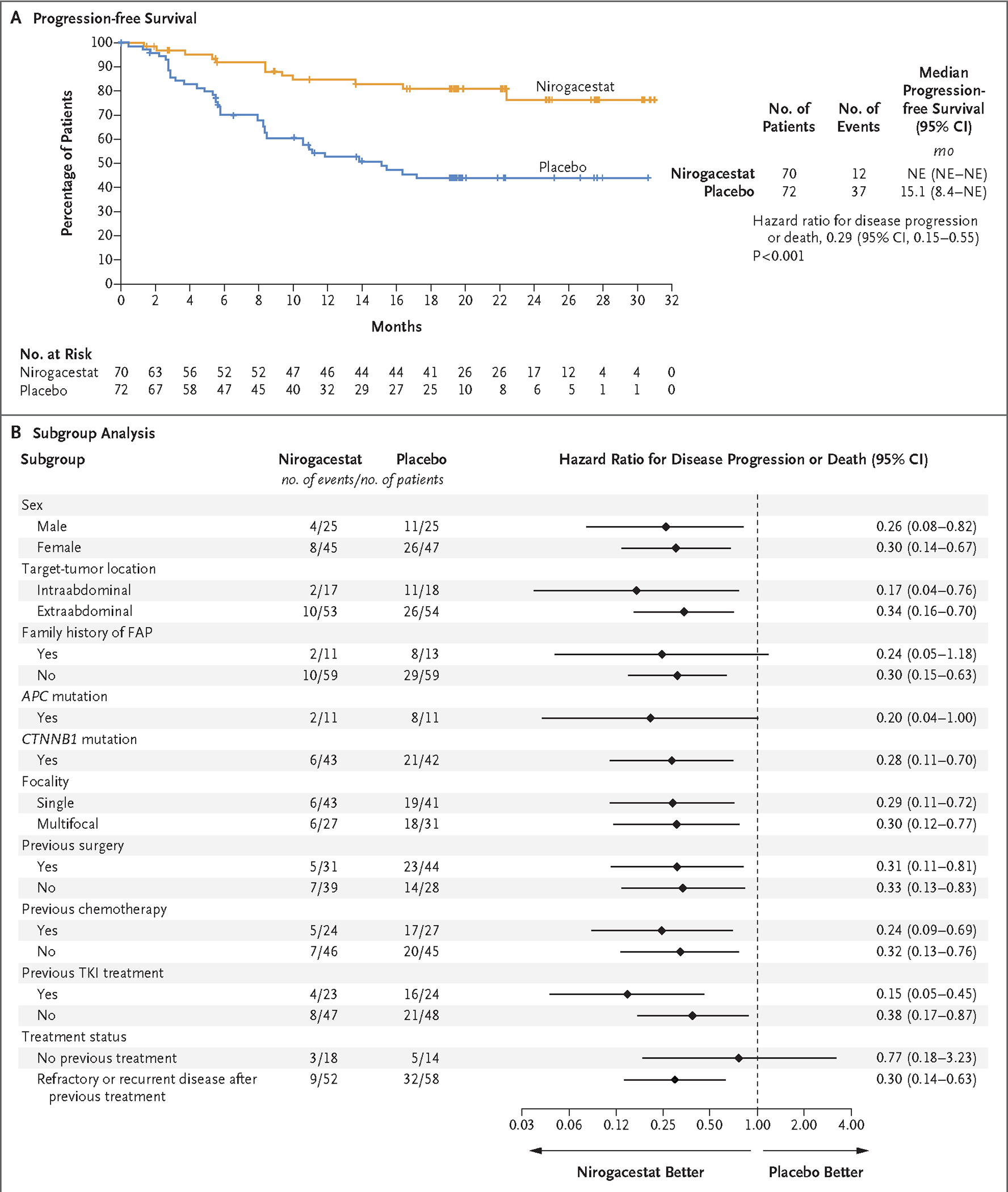
Methods: We conducted a phase 3, international, double-blind, randomized, placebo-controlled trial of nirogacestat in adults with progressing desmoid tumors according to the Response Evaluation Criteria in Solid Tumors, version 1.1. Patients were assigned in a 1:1 ratio to receive the oral γ-secretase inhibitor nirogacestat (150 mg) or placebo twice daily. The primary end point was progression-free survival.
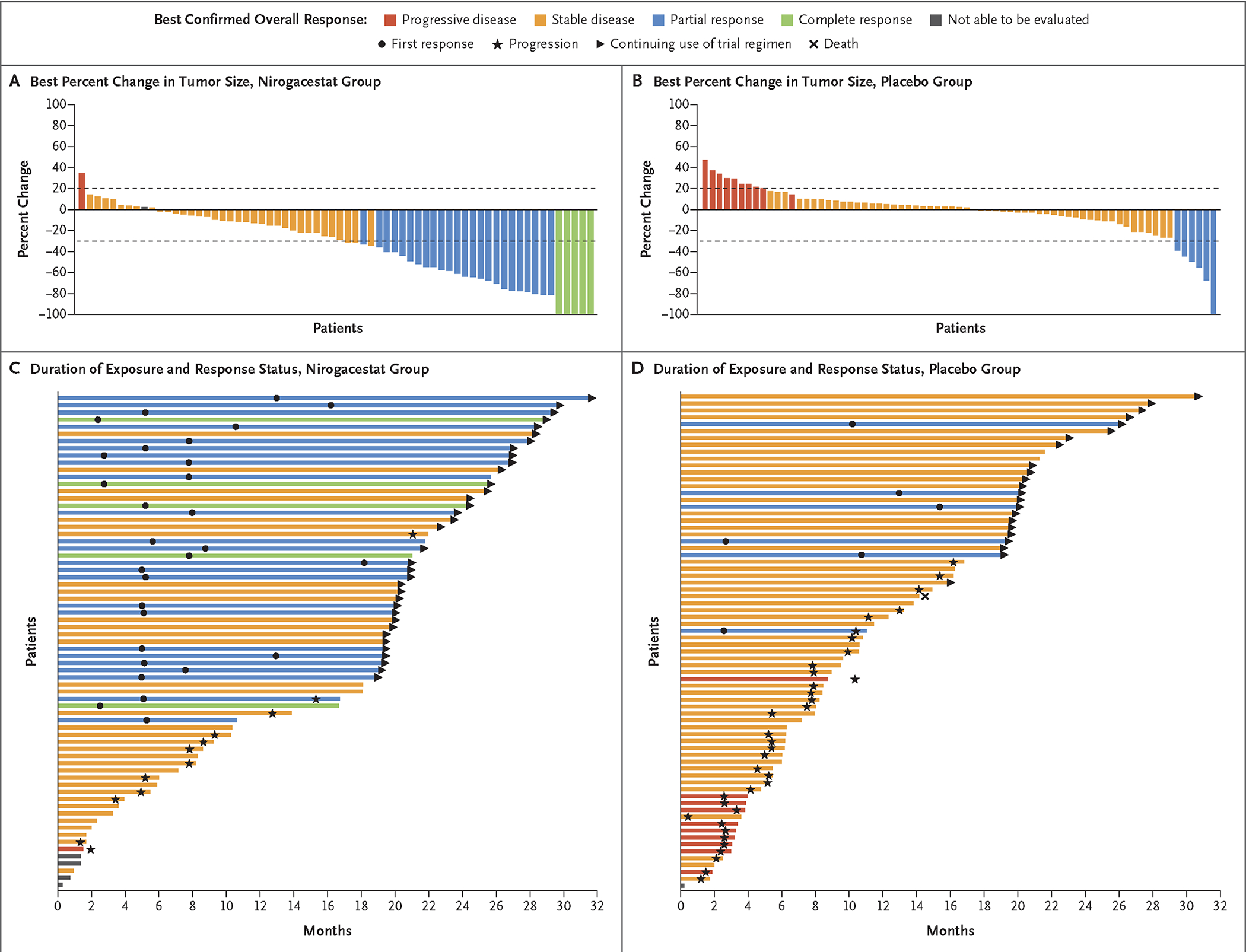
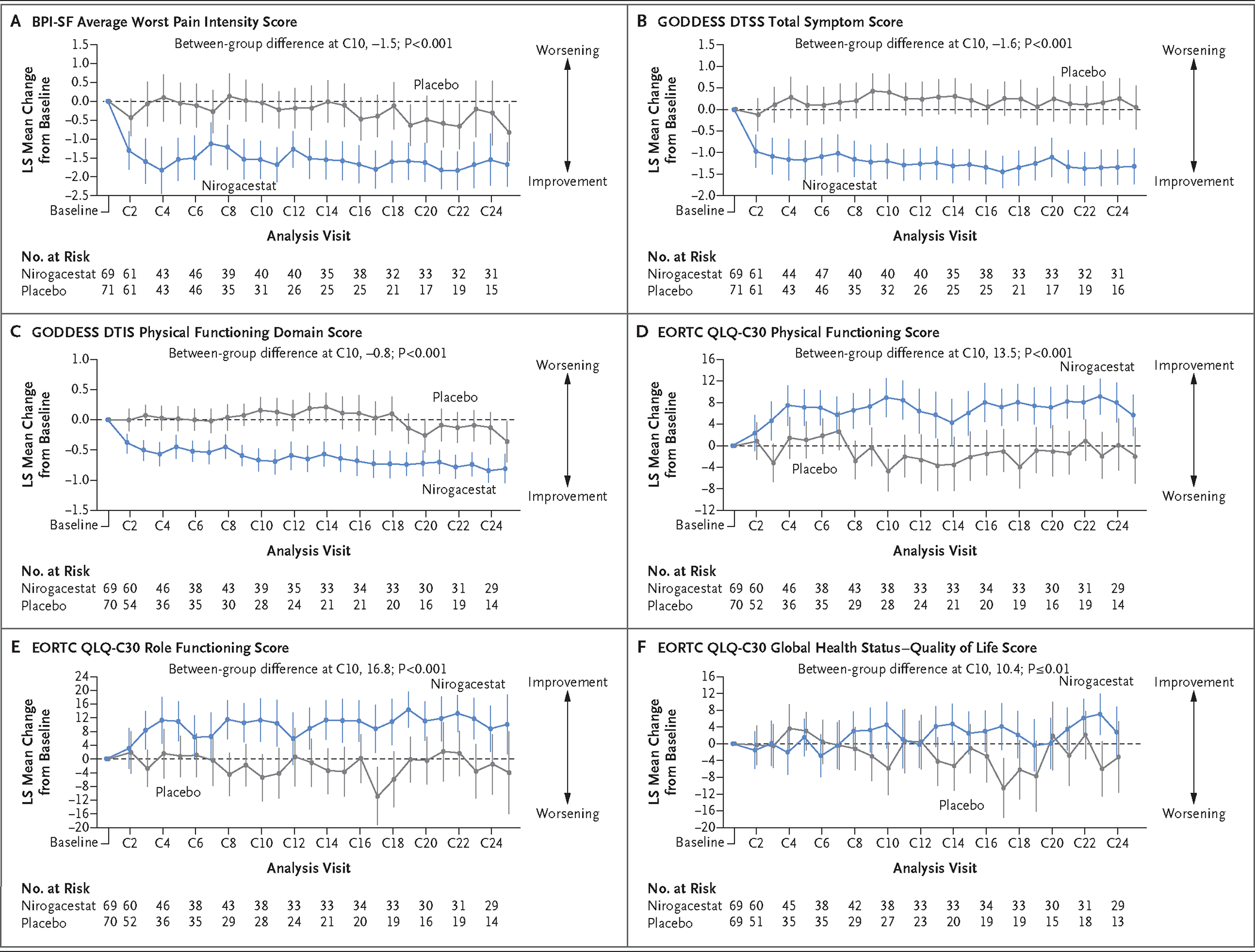
Results: From May 2019 through August 2020, a total of 70 patients were assigned to receive nirogacestat and 72 to receive placebo. Nirogacestat had a significant progression-free survival benefit over placebo (hazard ratio for disease progression or death, 0.29; 95% confidence interval, 0.15 to 0.55; P<0.001); the likelihood of being event-free at 2 years was 76% with nirogacestat and 44% with placebo. Between-group differences in progression-free survival were consistent across prespecified subgroups. The percentage of patients who had an objective response was significantly higher with nirogacestat than with placebo (41% vs. 8%; P<0.001), with a median time to response of 5.6 months and 11.1 months, respectively; the percentage of patients with a complete response was 7% and 0%, respectively. Significant between-group differences in secondary patient-reported outcomes, including pain, symptom burden, physical or role functioning, and health-related quality of life, were observed (P≤0.01). Frequent adverse events with nirogacestat included diarrhea (in 84% of the patients), nausea (in 54%), fatigue (in 51%), hypophosphatemia (in 42%), and maculopapular rash (in 32%); 95% of adverse events were of grade 1 or 2. Among women of childbearing potential receiving nirogacestat, 27 of 36 (75%) had adverse events consistent with ovarian dysfunction, which resolved in 20 women (74%).
Conclusions: Nirogacestat was associated with significant benefits with respect to progression-free survival, objective response, pain, symptom burden, physical functioning, role functioning, and health-related quality of life in adults with progressing desmoid tumors. Adverse events with nirogacestat were frequent but mostly low grade. (Funded by SpringWorks Therapeutics; DeFi ClinicalTrials.gov number, NCT03785964.).
Copyright © 2023 Massachusetts Medical Society.
Figures
Comment in
-
Nirogacestat effective in desmoid tumours.Nat Rev Clin Oncol. 2023 May;20(5):284. doi: 10.1038/s41571-023-00758-x. Nat Rev Clin Oncol. 2023. PMID: 36997640 No abstract available.
References
-
- Kasper B, Baumgarten C, Garcia J, et al. An update on the management of sporadic desmoid-type fibromatosis: a European Consensus Initiative between Sarcoma PAtients EuroNet (SPAEN) and European Organization for Research and Treatment of Cancer (EORTC)/Soft Tissue and Bone Sarcoma Group (STBSG). Ann Oncol 2017;28:2399–408. - PMC - PubMed
-
- Constantinidou A, Scurr M, Judson I, Litchman C. Clinical presentation of desmoid tumors. In: Litchman C, ed. Desmoid tumors. Dordrecht, the Netherlands: Springer Dordrecht, 2012:5–16.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical