

Cancer Treatment-Related Ovarian Dysfunction in Women of Childbearing Potential: Management and Fertility Preservation Options
- PMID: 36888938
- PMCID: PMC10115556
- DOI: 10.1200/JCO.22.01885
Cancer Treatment-Related Ovarian Dysfunction in Women of Childbearing Potential: Management and Fertility Preservation Options
Abstract
Purpose: To review the complex concerns of oncofertility created through increased cancer survivorship and the long-term effects of cancer treatment in young adults.
Design: Review chemotherapy-induced ovarian dysfunction, outline how fertility may be addressed before treatment initiation, and discuss barriers to oncofertility treatment and guidelines for oncologists to provide this care to their patients.
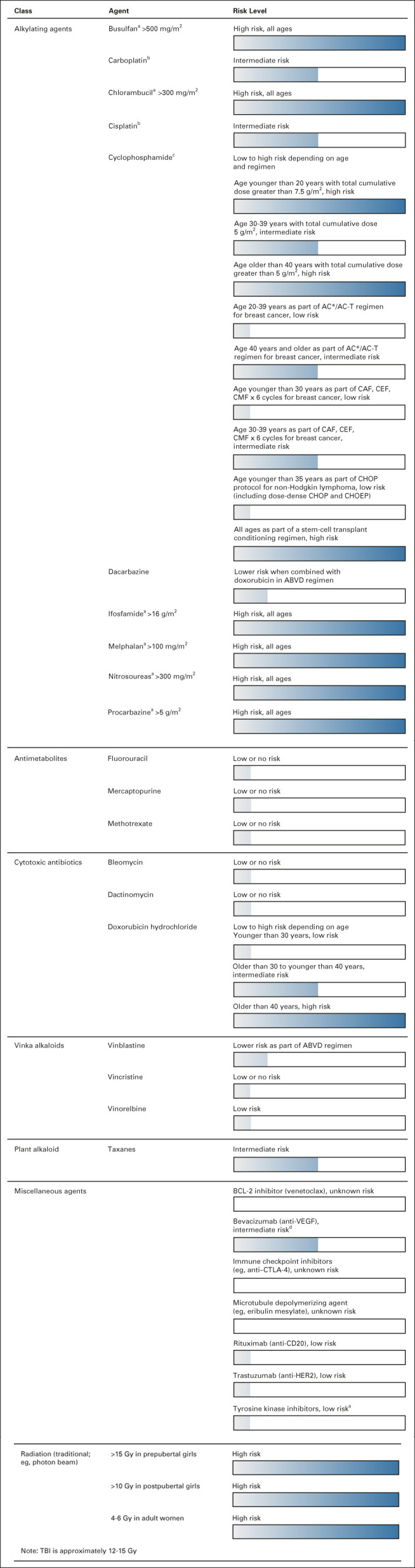
Conclusion: In women of childbearing potential, ovarian dysfunction resulting from cancer therapy has profound short- and long-term implications. Ovarian dysfunction can manifest as menstrual abnormalities, hot flashes, night sweats, impaired fertility, and in the long term, increased cardiovascular risk, bone mineral density loss, and cognitive deficits. The risk of ovarian dysfunction varies between drug classes, number of received lines of therapy, chemotherapy dosage, patient age, and baseline fertility status. Currently, there is no standard clinical practice to evaluate patients for their risk of developing ovarian dysfunction with systemic therapy or means to address hormonal fluctuations during treatment. This review provides a clinical guide to obtain a baseline fertility assessment and facilitate fertility preservation discussions.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
No other potential conflicts of interest were reported.
Figures
Similar articles
-
Approaches to Fertility Preservation for Young Women With Breast Cancer.Clin Breast Cancer. 2023 Apr;23(3):241-248. doi: 10.1016/j.clbc.2023.01.006. Epub 2023 Jan 14. Clin Breast Cancer. 2023. PMID: 36710145 Review.
-
Fertility preservation options in breast cancer patients.Gynecol Endocrinol. 2015;31(11):846-51. doi: 10.3109/09513590.2015.1081684. Epub 2015 Sep 15. Gynecol Endocrinol. 2015. PMID: 26370157 Review.
-
Strategies for fertility preservation in young early breast cancer patients.Breast. 2014 Oct;23(5):503-10. doi: 10.1016/j.breast.2014.05.024. Epub 2014 Jun 13. Breast. 2014. PMID: 24934638 Review.
-
Anticancer treatments and female fertility: clinical concerns and role of oncologists in oncofertility practice.Expert Rev Anticancer Ther. 2017 Aug;17(8):687-692. doi: 10.1080/14737140.2017.1335199. Epub 2017 Jun 5. Expert Rev Anticancer Ther. 2017. PMID: 28537815 Free PMC article. Review.
-
Recent advances in fertility preservation and counseling for female cancer patients.Expert Rev Anticancer Ther. 2018 Feb;18(2):115-120. doi: 10.1080/14737140.2018.1415758. Epub 2017 Dec 15. Expert Rev Anticancer Ther. 2018. PMID: 29220203
Cited by
-
Ameliorative Effect of Chitosan/Spirulina platensis Ethanolic Extract Nanoformulation against Cyclophosphamide-Induced Ovarian Toxicity: Role of PPAR-γ/Nrf-2/HO-1 and NF-kB/TNF-α Signaling Pathways.Mar Drugs. 2024 Aug 30;22(9):395. doi: 10.3390/md22090395. Mar Drugs. 2024. PMID: 39330276 Free PMC article.
-
A Representative Clinical Course of Progression, with Molecular Insights, of Hormone Receptor-Positive, HER2-Negative Bone Metastatic Breast Cancer.Int J Mol Sci. 2024 Mar 17;25(6):3407. doi: 10.3390/ijms25063407. Int J Mol Sci. 2024. PMID: 38542380 Free PMC article. Review.
-
Gynotoxic Effects of Chemotherapy and Potential Protective Mechanisms.Cancers (Basel). 2024 Jun 20;16(12):2288. doi: 10.3390/cancers16122288. Cancers (Basel). 2024. PMID: 38927992 Free PMC article. Review.
-
Effects of Chemotherapy on Fertility and Fertility Preservation Strategies for the Women of Childbearing Potential Undergoing Chemotherapy: A Comprehensive Review.Indian J Surg Oncol. 2025 Apr;16(2):401-407. doi: 10.1007/s13193-024-02103-9. Epub 2024 Sep 26. Indian J Surg Oncol. 2025. PMID: 40337032 Review.
-
AMH decline during chemotherapy reflects breast cancer cell DNA damage response (DDR) proficiency: the ONCO AMH1 pilot study.J Assist Reprod Genet. 2025 May;42(5):1435-1441. doi: 10.1007/s10815-025-03475-9. Epub 2025 Apr 12. J Assist Reprod Genet. 2025. PMID: 40220108 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
