

Strength of association between comorbidities and asthma: a meta-analysis
- PMID: 36889783
- PMCID: PMC10032614
- DOI: 10.1183/16000617.0202-2022
Strength of association between comorbidities and asthma: a meta-analysis
Erratum in
-
"Strength of association between comorbidities and asthma: a meta-analysis" Paola Rogliani, Rossella Laitano, Josuel Ora, Richard Beasley and Luigino Calzetta. Eur Respir Rev 2023; 32: 220202.Eur Respir Rev. 2023 Jun 7;32(168):225202. doi: 10.1183/16000617.5202-2022. Print 2023 Jun 30. Eur Respir Rev. 2023. PMID: 37286222 Free PMC article. No abstract available.
Abstract
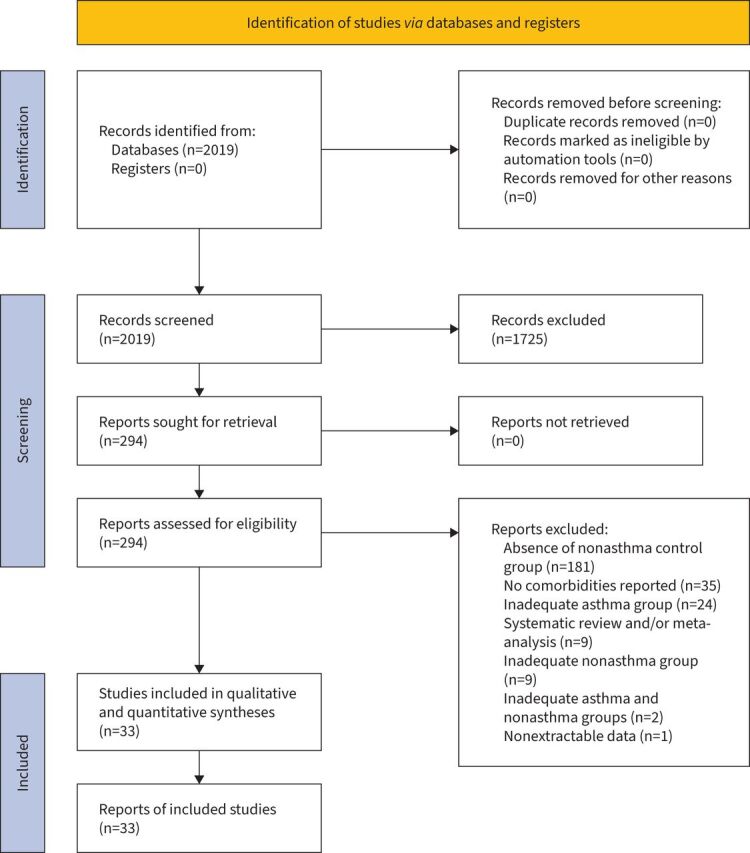
Background: The strength of association between comorbidities and asthma has never been ranked in relation to the prevalence of the comorbidity in the nonasthma population. We investigated the strength of association between comorbidities and asthma.
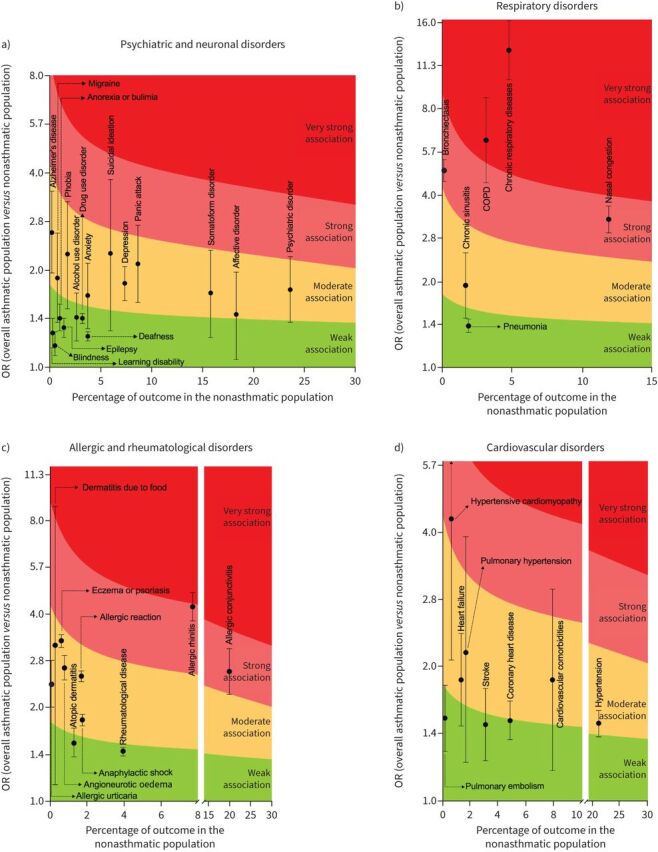
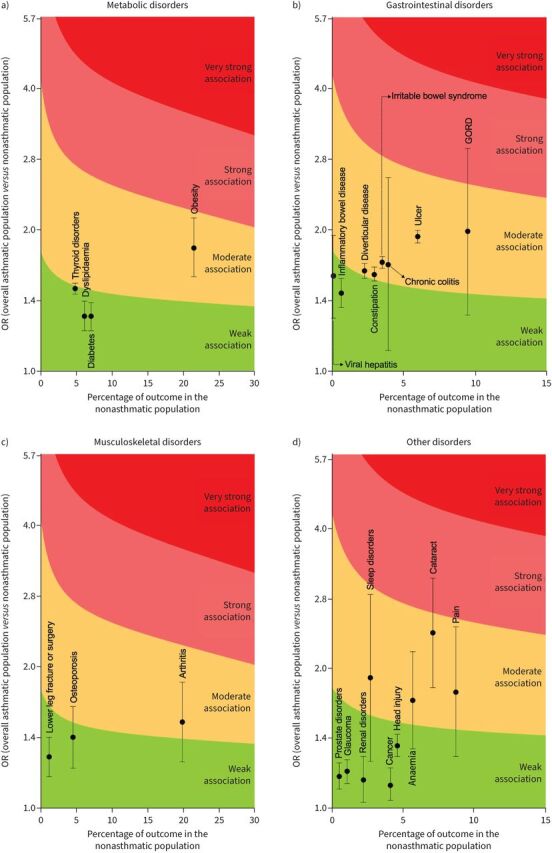
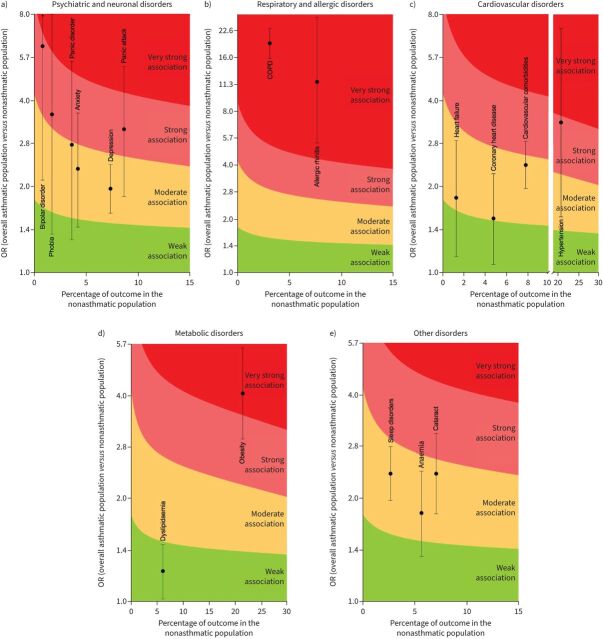
Methods: A comprehensive literature search was performed for observational studies reporting data on comorbidities in asthma and nonasthma populations. A pairwise meta-analysis was performed and the strength of association calculated by anchoring odds ratios and 95% confidence intervals with the rate of comorbidities in nonasthma populations via Cohen's d method. Cohen's d=0.2, 0.5 and 0.8 were cut-off values for small, medium and large effect sizes, respectively; very large effect size resulted for Cohen's d >0.8. The review was registered in the PROSPERO database; identifier number CRD42022295657.
Results: Data from 5 493 776 subjects were analysed. Allergic rhinitis (OR 4.24, 95% CI 3.82-4.71), allergic conjunctivitis (OR 2.63, 95% CI 2.22-3.11), bronchiectasis (OR 4.89, 95% CI 4.48-5.34), hypertensive cardiomyopathy (OR 4.24, 95% CI 2.06-8.90) and nasal congestion (OR 3.30, 95% CI 2.96-3.67) were strongly associated with asthma (Cohen's d >0.5 and ≤0.8); COPD (OR 6.23, 95% CI 4.43-8.77) and other chronic respiratory diseases (OR 12.85, 95% CI 10.14-16.29) were very strongly associated with asthma (Cohen's d >0.8). Stronger associations were detected between comorbidities and severe asthma. No bias resulted according to funnel plots and Egger's test.
Conclusion: This meta-analysis supports the relevance of individualised strategies for disease management that look beyond asthma. A multidimensional approach should be used to assess whether poor symptom control is related to uncontrolled asthma or to uncontrolled underlying comorbidities.
Copyright ©The authors 2023.
Conflict of interest statement
Conflict of interest: P. Rogliani participated as a lecturer and advisor in scientific meetings and courses under the sponsorship of Almirall, AstraZeneca, Biofutura, Boehringer Ingelheim, Chiesi Farmaceutici, GlaxoSmithKline, Menarini Group, Mundipharma, and Novartis, and her department was funded by Almirall, Boehringer Ingelheim, Chiesi Farmaceutici Novartis, and Zambon, outside the submitted work. Conflict of interest: R. Laitano has nothing to disclose. Conflict of interest: J. Ora has nothing to disclose. Conflict of interest: R. Beasley reports grants and personal fees from AstraZeneca, grants from GlaxoSmithKline and Genentech, personal fees from Avillion and Theravance, outside the submitted work. Conflict of interest: L. Calzetta has participated as advisor in scientific meetings under the sponsorship of Boehringer Ingelheim and Novartis; received nonfinancial support from AstraZeneca; a research grant partially funded by Chiesi Farmaceutici, Boehringer Ingelheim, Novartis, and Almirall; is or has been a consultant to ABC Farmaceutici, Edmond Pharma, Zambon, Verona Pharma, and Ockham Biotech; and his department was funded by Almirall, Boehringer Ingelheim, Chiesi Farmaceutici, Novartis, and Zambon, outside the submitted work.
Figures
References
-
- World Health Organization (WHO) . Asthma. www.who.int/news-room/fact-sheets/detail/asthma. Date last accessed: 22 February 2022.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical